SirBillybob
-
Posts
3,825 -
Joined
-
Last visited
Content Type
Forums
Donations
News
Events
Gallery
Everything posted by SirBillybob
-
What fun for a nerd. Andy Carstens, who by the way did not source his breakthrough infection case reports, would have been well advised to do his homework, reading in fact research reported a substantial period of time prior to his article date. It is likely his estimate was derived from a search of individual case reports that clinicians here and there bothered to submit, probably not structured cohort surveillance. One cannot know because the information is missing. It smacks of confirmation bias. Expected real world infection breakthrough extrapolated from prospective study model surveillance is estimated as 1,500 per million consumers for Apretude over a year, 150-fold the erroneous waaaaay off the mark Aidsmap summation (non-adjusted by time and non-specific uptake mode, as they are episodic cases), and then translating to 1 in 133 over 5 years, and then yet a further 3-fold degree for Truvada. It is more accurate because it follows the same cohort given PrEP. See appended media piece. As I wrote above, retrospective case control research, wherein rates of historical oral PrEP uptake, with appropriate data-censoring following discontinuation, are compared between those later seroconverting and those counterparts that remained HIV negative, matched across key demographic characteristics, yielded poor effectiveness results. In contrast to the aforementioned randomized trial depicting 15 breakthrough cases per 10,000 person years, case control results about 22 cases per 10,000 person years, about 29% of infections PrEP users. Of course PrEP is superior to not being on it. That is the relation between intervention and nothing. It will reduce infection risk, no argument. Questioning and appraising the apparent hyperbole associated with effectiveness simply represents appreciative inquiry however much it spurs hyperventilation response. That part is the relation between an intervention and within-group case incidence. No need to go to the mat. The thread topic pertains to the downstream reality of delineating PrEP status. Breakthrough HIV reported in injectable PrEP trial; experts say drug still very effective WWW.NBCNEWS.COM Experts say breakthrough HIV should still remain rare in those receiving ViiV Healthcare’s...
-
It’s very poor real world effectiveness -wise in nested case-control study for behaviourally high-risk men (ie, STI occurrence corroborating condom practices) younger than 30 that report categorical use of oral PrEP … about 25% effective, not differentiating insertive from receptive anal. In fact the low end of the metric confidence interval for that age group drops below nil efficacy. HIV incidence is much much lower than overall STI incidence but oral PrEP certainly has its limits. For men over 40, real world effectiveness is much better, approaching that of randomized placebo-control research. Given typical punter-scort age differential the prevention key is client PrEP uptake. That said, synergistic assumptions such as enhanced protection conferred by mutual categorical PrEP use should be made with a grain of salt, condom use making up the efficacy gap according to risk tolerance. At some future point, fingers crossed, the long-lasting depot injection PrEP model may prove to be a real world game-changer.
-
😊Likely a mix of values, resolve, the good fortune of non-chronicity, and constitutional hypersensitivity. First time pot, barf. That was it. First time moderately inebriated drinking far less than peers, barf. Never again. First time Fentanyl-inclusive monitored anaesthesia for hernia repair, barf barf barf 10 seconds after coming to in wheelchair; team rushed in with IM injection. Fortunately surgeon was steps away on lunch break rather than mid-procedure the next patient. A health care colleague is a renowned pain management psychologist and I would likely seek a referral for non-pharmacological intervention if it came to it, though expensive and non-insured. Or get into a study. I am sure stoicism has its limits and blending that approach with meds a possible eventuality. But, right, Dopesick is certainly heartbreaking.
-
Man I’ve been there. Commiserations. Yeah the 30mg of codeine added to acetaminophen (prescription) really makes a difference taken at bedtime, and I am convinced that it plays a major role in returning to zero pain baseline. I have rarely needed it more than two consecutive nights a few times yearly and I take the almost full bottle to my annual medical exam to demonstrate lack of dependency.
-
Or health promotion conditions like HIV negative and protected sex. Not exactly unicorns in my microcosm of the world. Like I suggested, the discussion gateway potential overrides the good intentions gone partially bad.
-
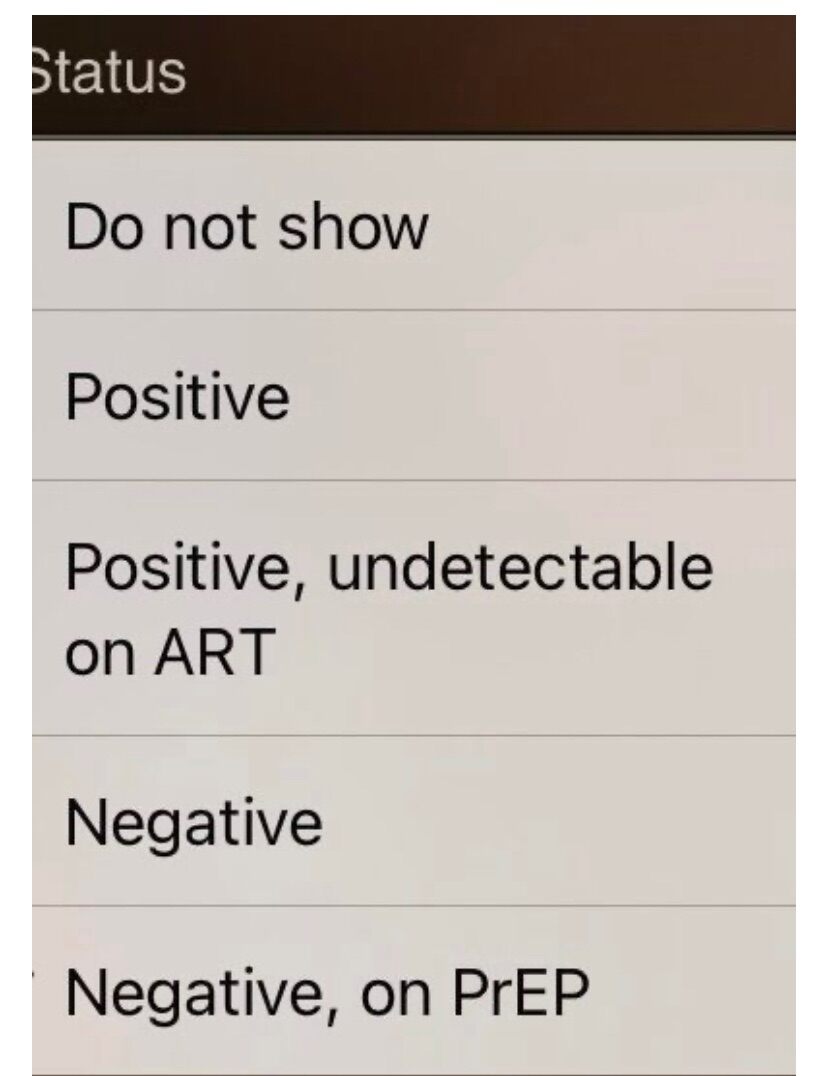
The categorization is overly simplistic, so the ad platform offers the info opt-out. The drop-down field is designed to stimulate rapport, to support that it is normative to maturely discuss STI topics. The provider will have explicitly chosen among status choices, albeit not all semantically fully accurate. If it is blank he had nevertheless decided to redact the info. Therefore, an inquiry opening up the topic will (should) not be out of left field as it was formally kick-started upon ad registration.

-
Do you think it was an identifiable injury from some kind of exertion or that the musculature cluster just basically went into spasm spontaneously, like a mind of its own, releasing chemicals that irritate the nerve group? The latter occurs for me occasionally. Past week I think triggered by tensing up when wearing heavier clunky footwear on icy walkways. Max discomfort tends to be when getting out of bed after a nap or full night’s sleep. Things I do: Walk it off, trying to keep surrounding muscle groups loose, as opposed to staying immobile. Tylenol-3, usually max 2 or 3 per episode, cumulatively half a dozen tabs annually, but when taking time to rest as they promote drowsiness. Continue more peripheral resistance training at the gym, but not focused core exertion. Sounds counterintuitive but helps. Today I did my full chest & upper back routine. Also stretch, with emphasis on hamstrings, as all muscle groups are implicated in spontaneous sciatic spasm. That said, such activity is based on lack of evidence of the problem having been triggered by exertion such as heavy lifting in a bad position. I feel nerve pain, not muscle discomfort. In other words, I only know the spasm exists due to nerve irritation and body line nude in the mirror is a bit off. Apply external Thumper Massager which my effective chiropractor of years back, now retired, used on me in treatments, along with a rolling pin (his playbook; I use a foam roller and slide on it under me). He had put little emphasis on conventional adjustment manoeuvres. Hot pool water jets directly on the area at Spa Scandinave in Old Montreal. Very effective but the jets must be extremely robust, so that I gently anchor myself as they propel my floating body away from the jet flow. I find it’s the most effective mitigator.
-
À chacun son goǔt. I live in Montreal and have a nice centrally located place to host but the inventory is just not here. Up until 15 years ago, though, many outcalls from strip club dancers when strippers were all that. I now commute to Toronto, where I worked for 4 decades, for a regular, exclusively for meeting up. I must admit I have never committed to visiting Toronto for an ad-based fellow. Only drawing from Onlyfans, tipping, progressing from there. However, IMHO the array of Toronto ads seems overall more appealing than my current home city. Nothing about any of the few photos posted in this thread impels me to tap into Toronto further. Luckily, my workaholism in Toronto in its day was rewarded with off-venue talent from Remington’s and BrassRail’s weekly Heaven. Sigh. Now for about twice the travel time Spain and Brazil constantly beckon, arrangements success at one’s fingertips.
-
That’s usually a cover for grandmother fracturing her tibia doing motorcycle wheelies and needing to get to her in urgent care.
-
Waterloo? Napoleon complex? May have abruptly run out of keypad blackberries to click or the heart emoticon finally crashed it.
-
Hydrate. It’s free, the least you can do, the most you can do for seminal fluid volume, and the only do I’d recommend. Otherwise, the list is comprised of don’ts, eg, smoking, poor diet, etc, that negatively correlate with ejaculatory robustness. Also be aware of the distinction between semen and sperm in terms of influence targets.
-

Currently not hiring due to lack of interest?
+ SirBillybob replied to acks0104's topic in Questions About Hiring
Out of Bordeaux nothing wrong with a full-bodied Pinot Gigolo. -
Currently not hiring due to lack of interest?
+ SirBillybob replied to acks0104's topic in Questions About Hiring
Au contraire. Local would be my preference and I search ad databases at least weekly. It’s not a principle. I was following the thread’s train of thought. -
-
For men age 27-45 is the ‘shared patient-physician clinical decision-making’ range, and 46+ is not recommended based on a number of factors including likely past exposure and unlikely high number of partners going forward. It would be imperative that he disclose his risk factors as distinct from the more monogamish-prone average middle-aged adult. There is evidence to support vaxx for women >45 but it is due to an inexplicable secondary peak risk of infection in that age range. No clinical evidence to support vaxx for men >27 but practice wisdom suggests that MSM are good candidates as risk is 20-fold, and suggests that age need not be a relevant factor; no clear distinction in MSM age stratification 27-45 vs >45. The upper age limit 45 for discretionary uptake for the general population may yet increase in terms of eligibility guidance; vaccination is not contraindicated due to any age-based safety reason. It is an arbitrary age cut-off. Survey says yes?
-
Currently not hiring due to lack of interest?
+ SirBillybob replied to acks0104's topic in Questions About Hiring
-
Beyond Judith Smith’s small but promising American placebo-control AHCC study of 41 adult women published almost 2 years ago there is only one other ongoing similar trial, in China, with results not anticipated for at least another year. That said, I might be inclined to take it on preliminary ‘proof of concept’ merit. Oddly, no p value explicitly calculated but I computed the chi-squared as .029, acceptably below the .05 threshold. Trouble is that the sample size is so small that merely either one more favourable individual outcome among the placebo group or one less favourable outcome among the treatment group fails to meet the standard for statistical significance of difference. The clinical significance is reasonable. The devil is in the details.
-
Fake. Only two 6’s in the phone #.
-
Yes, more disposable funds beyond nest-egg target.
-
Currently not hiring due to lack of interest?
+ SirBillybob replied to acks0104's topic in Questions About Hiring
For me, a quality deficiency not funds. I just discovered, without specifically looking, that there are more than 7,000 client profiles in my metro area of 3-ish million registered with Rentmen. As we know, that could be the tip of the iceberg as you don’t need an account to reach most advertisers. I don’t hire from the platform because the profiles, in contrast to some other regions, don’t interest me. I spend more than $400 on average including provider rate per desirable hire to travel significant distances to them, usually at least 10 hours one way. I keep open to enjoying the destinations but would otherwise not visit for the most part, preferring to explore new locations in which hiring would not be on the table. However, now I grasp that those among the huge volume of potential clients could be hiring from local listings such that all are getting some business. -
Yes.
-
I had planned to attend on a Friday or Saturday out of curiosity but changed my mind, as the time difference makes being up that late more manageable, but not 05:00! They run four nights Thursday-Sunday, have been for several months. The ‘word on the street’ is that the events are barely attended from 23:00 for a few hours, even Friday and Saturday, and that customers begin to trickle in around 03:00 when bars close and they are choosing this over other clubs that serve until 06:00, and the DJ may commence around 05:00 as opposed to continuously from 23:00, so patterns attributable to partiers finishing up elsewhere and then moving on to this regularly occurring event. Things can get very busy as late as 07:00 and through the morning, perhaps as club-goers in places closing at 06:00 are not ready to head home. If you prevail upon the courtesy of entrance booth staff you can be informed about the approximate number of attendees prior to committing, as per usual. Attendees optionally hook up in a conventional bathhouse manner. There seem to be some experiments in pricing time blocks and some offer an inclusive ticket (actually a #, perhaps same as locker) for a drink. The idea is to charge from 23:00 covering up to the final afternoon, or at times a separate charge from 05:00 on for those arriving really late, then the historical rates beginning afternoons. I think that if a customer wishes to stay for the afternoon and evening they would need to pay the historical day rate even if they had attended the previous party leading in. Otherwise, there is no interference between the two, and there is an agenda division according to the two categories of clientele, with historical afternoons/evenings business as usual. Simply put, the premises are put to more full-time use.
-
A message from King Charles III: check your prostate!
+ SirBillybob replied to marylander1940's topic in Men's Health
Purely speculative, as there are several procedures that could justify extended convalescence, but that might put a princess in colostomy or ileostomy territory, with possible reversal down the line. My cousin had such, not cancer, with subsequent reversal, and she’s healthy 35 years on. Imagine the endless relentless joking in poor taste, though. One wonders if the omission of specificity around Charles’ BPH procedure, where a good reason for ambiguity may be lacking since the release is partly geared to men’s health education, is intended to mirror for the sake of content consistency the level of confidentiality regarding his daughter-in-law’s surgery. -
The Ups and Downs of Airlines and Air Travel
+ SirBillybob replied to mike carey's topic in The Travel Desk
Non-stop gay?
-
The Ups and Downs of Airlines and Air Travel
+ SirBillybob replied to mike carey's topic in The Travel Desk
IATA mind yer Ps and Qs, Ms Noma.