SirBillybob
-
Posts
3,825 -
Joined
-
Last visited
Content Type
Forums
Donations
News
Events
Gallery
Everything posted by SirBillybob
-
Interesting and important question. Short answer: A lot of complex variables are involved in second-guessing timeline for the Novavax formulation. I will touch on a few. Note that none of the 3 are technically boosters. They are designed as if the ancestral CoV strain in well behind us. Therefore, the standards of viability are as stringent as a few years ago for the initial candidates. That said, track records and vaccine platform preferences are likely ‘unofficially’ folded in to authorization decisions. Novavax is historically plagued with being bridesmaid, option of last resort, go-to choice of mRNA hesitancies, &c. I don’t need inoculation now but I would have no problem choosing Nuvaxovid re-boot. That said, I am Team Whatever Is Approved. All 3 companies presented to CDC’s immunization advisory committee on 12 Sept, a day following FDA approval of both Pfizer and Moderna. So the two mRNA options already had it in the bag. Moderna is recently approved in Canada while Pfizer awaits disposition. The two are essentially viewed as interchangeable. My sense is that the trajectory of non-clinical or pre-clinical (ie, animal models of immune response) progressing to human data confers an edge. Novavax has presented macaque immunogenicity data. As I put elsewhere they are still recruiting for their human immunogenicity trial and all subjects (N=330?) will get the new vaccine. If desired, I can steer those interested but it helps to know if study site location will fit, and a few attendances and solid follow-up commitment are required. But no older than age 54. I think another hurdle for Novavax is the added demonstration of legitimacy for cross-platform, or what is called heterologous dosing. Most folks have had within-mRNA sequential dosing, termed homologous. The CDC meeting threw a question to Novavax regarding the introduction of heterologous dosing for a greater number of people having previous exclusive mRNA uptake. Homogolous and heterologous dosing are generally considered mutually non-inferior but there may be sticklers peppering authorization entities around this question. In sum, I would venture to forecast that Novavax access, although likely quick at getting from authorization to table, will not precede Turkey dinner or be stuffed into mantle stockings. In fact, it could be initially restricted to previous Nuvaxovid recipients. Its other two potentials are the heterologous model as described above with single-dose series or a 2-dose series for those completely unvaccinated to date.
-
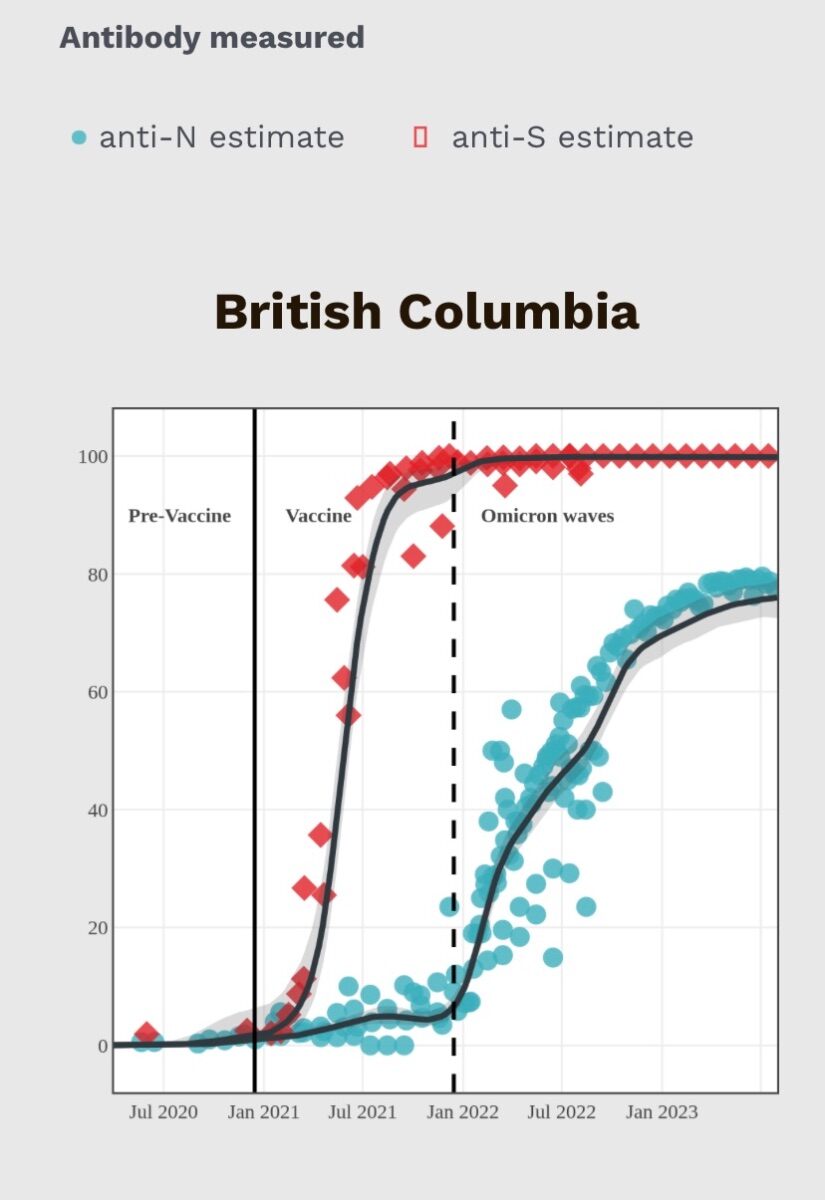
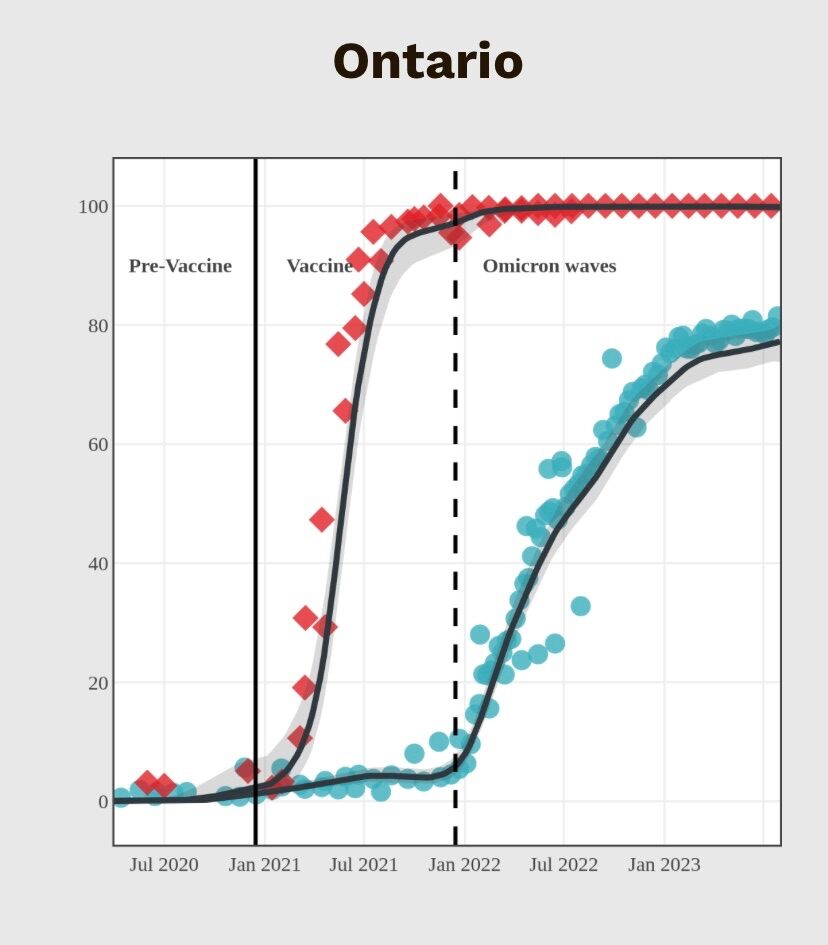
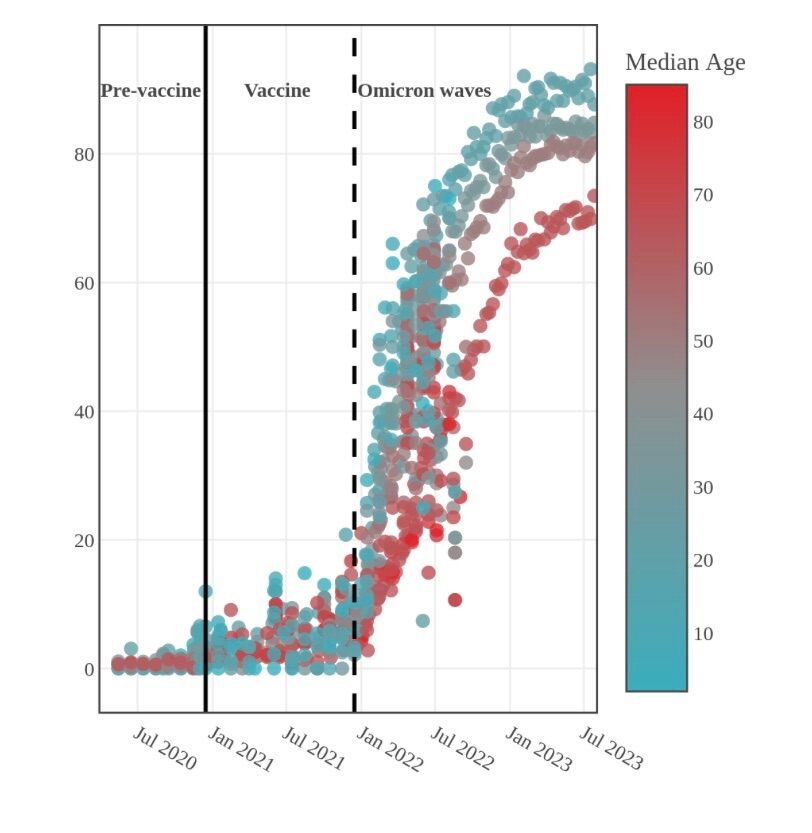
Let’s unpack this a bit more. In the absence of 2023 USA data, what immunity research might one draw on to estimate ongoing cumulative infection-induced N-antibody seroprevalence subsequent to the latest CDC slice some 9 months ago? I don’t have time to search global regional trends. In Canada we see a relative levelling off of increase in infection immunity rates by time throughout 2023. If it weren’t for a 10% increase among older folks, always in fact lagging behind in evidence of infection acquisition, the plateau or relative flattening trend would be more pronounced. I might dare to put forward that a similar increase to, say, 85% in USA trends will be borne out in the next analysis iteration. But none of us is a crystal-ball gazer. Geographic population density has been assessed a little but seemingly only in Quebec, with no difference in infection immunity between the two urban centres and the dozen or so less populated regions. In fact the sparser areas to date have higher rates of infection immunity but when looking at confidence intervals for the smaller sample sizes those differences are essentially nullified. I append 2 specific province graphs, and an age-based graph representing all of Canada for the N-antibody component. It doesn’t seem off base to assume that a substantial minority of board members, given age demographics, remain infection virgins, notwithstanding that both under-the-radar infection and spidey-sense are poor predictors of type of immunity. I am not an immunologist but I thought that over time, and given re-infection in terms of this disease, the residual minority of uninfected are not particularly low hanging fruit for first infection. Moreover, the extremely high rate of population artificial immunity in concert with ever increasing hybrid immunity would be a protective factor transmission-wise for the as yet infection-spared. That said, I am hacking through a sinus cold superimposed on a recent initial SARS-CoV infection characterized by transient high fever and now remitted aggravatingly itchy abdominal trunk flank rash of 2 weeks. I tracked my infection status microbiologically over the past few years and made the decision to defer a Fall Europe trip pending re-vaccination (now moot), so pandemic OCD sometimes pays off with respect to circumventing illness abroad. I am sleeping marvellously.

-
Last year I came across a few cross-affiliated fellows, at 50-ish in Thermas yet 150-ish via ad sites, the latter obviously more the full hour. Not surprising that some degree of gap closure would evolve. 75 in a structured environment with an expanded array of choice seems reasonable. What I am currently curious about is how much the apparently large volume of visiting providers with site ads might be supplementing in this manner, as some work in Spain seasonally, temporarily, even in cycles.
-
 Uncut is Director’s Cut topic prerogative. Personally, I think I tune in at times because he (you, J, are) is articulate but tune out due to a (my) sense of impotence with respect to influencing outcome. Fortunately, J frames these threads as potentially cathartic, so there’s that. And is not contemptuous towards the board membership largely made up of client constituency; I am sure some disgruntled providers have a major hate-on that they performatively mask. Unfortunately, while a variety of sound and interesting contributions here, some with supportive empathy, there’s little scope here for Dr Wendy Rhoades-grade job coaching, that is, as vocation dynamics can be complex in their own right and not necessarily attributable to personal deficiency. That said, the OP is bright and articulate, certainly not without potential, and a formidable focused baseline drive. Interestingly, the latest BILLIONS episode included our fave ex-marital-dom Wendy referencing Tversky and Kahneman. (Yeah, this gives away I utilize closed-caption😏.) Late last night I took to reading their dozen-page essay Judgement Under Uncertainty: Heuristics & Biases. It strikes me how the OP’s understandable uncertainty about how bookings will roll out, a wild snakes’n’ladders ride, runs up against the ambivalence and reservations about outcome probabilities that seems central to many prospective clients. The written piece also touches on the worthlessness of information that may be presented (in this case to clients) with good intentions but, as other posters opined, is best extremely edited and streamlined, IF the goal is deal-seal above and beyond process. Another concept is that of anchoring assumptions in such a way that other possibilities are overlooked. We perhaps see this within both our illustrious appellant and various contributions within the thread. Obviously, there is too much to summarize from the essay but my sense is that a paradigm shift, as also put forward by others, is necessitated here in order to acquire a sustainable stroke exceeding head above water.
Uncut is Director’s Cut topic prerogative. Personally, I think I tune in at times because he (you, J, are) is articulate but tune out due to a (my) sense of impotence with respect to influencing outcome. Fortunately, J frames these threads as potentially cathartic, so there’s that. And is not contemptuous towards the board membership largely made up of client constituency; I am sure some disgruntled providers have a major hate-on that they performatively mask. Unfortunately, while a variety of sound and interesting contributions here, some with supportive empathy, there’s little scope here for Dr Wendy Rhoades-grade job coaching, that is, as vocation dynamics can be complex in their own right and not necessarily attributable to personal deficiency. That said, the OP is bright and articulate, certainly not without potential, and a formidable focused baseline drive. Interestingly, the latest BILLIONS episode included our fave ex-marital-dom Wendy referencing Tversky and Kahneman. (Yeah, this gives away I utilize closed-caption😏.) Late last night I took to reading their dozen-page essay Judgement Under Uncertainty: Heuristics & Biases. It strikes me how the OP’s understandable uncertainty about how bookings will roll out, a wild snakes’n’ladders ride, runs up against the ambivalence and reservations about outcome probabilities that seems central to many prospective clients. The written piece also touches on the worthlessness of information that may be presented (in this case to clients) with good intentions but, as other posters opined, is best extremely edited and streamlined, IF the goal is deal-seal above and beyond process. Another concept is that of anchoring assumptions in such a way that other possibilities are overlooked. We perhaps see this within both our illustrious appellant and various contributions within the thread. Obviously, there is too much to summarize from the essay but my sense is that a paradigm shift, as also put forward by others, is necessitated here in order to acquire a sustainable stroke exceeding head above water. -
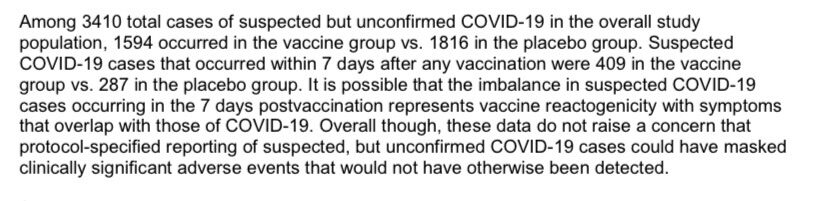
The purpose of immunization would be the possibility that anyone and everyone could acquire viral infection but that artificial immunity would render natural immune response a much less rough journey. Natural immune response, infection-induced, to date is estimated as 80% of the total population. In fact PfizerBNT’S FDA submission late 2020 reported a suspected rate of SARS-CoV-2 infection in the vaccine group that was 150 times that of case count used in efficacy computation (see insert below). That metric would not be dissimilar to the pre-vaccination general population incidence at the time. It would have been cost-prohibitive and extremely impractical to track infection-induced nucleocapsid protein antibody production precipitated by actual infection, in order to differentiate hybrid immunity from artificial immunity among those vaccinated in the trial, and in order to differentiate natural immunity from infection-spared among placebo recipients. The key was to demonstrate protection from serious illness and get a viable vaccine on the table. Vaccination was not designed to prevent viral exposure and natural immunity. The reality of a current majority of the population having acquired infection, with far less dire consequences, simply supports the legitimacy of vaccination development and administration efforts made to get there. I don’t grasp negative spins on this, though it is well established that the illusion of opinion validity is unequally distributed.
-
These CDC data are entirely consistent with Canada’s Immunity Task Force findings, up to and including July 2023, so ours slightly higher in the categorical nucleocapsid antibody rates that signify infection, as I indicated above.
-
Quebec City is so gorgeous in the Fall and it is easy to navigate, walkable-wise, the main sights in merely 2-3 days. Both lower town and upper town. Perhaps use more financial resources for upscale gastronomie in lieu of danseurs nus.
-
There is no strip club or bar with male strippers in Quebec City.
-
What's considered acceptable medical care in your country?
+ SirBillybob replied to a topic in Men's Health
Formal surveillance shows that NHS patient satisfaction is at an all time low. That said, I am surprised an Ophthalm consult wasn’t in the cards. In contrast to Ontario where I lived most of my adult life, in Quebec I pay out of pocket for primary care and urology, both practitioners having ‘opted out’ as is legal here; lab work, and MRI imaging. None of it is tax-credited due to my income level. I have had a few ultrasounds and dermatology check-ups covered by provincial health insurance. STI testing is covered at community clinics; as an active gay man I feel that is a good compensatory offset. I have travelled abroad specifically for specialty inguinal hernia repair accessed on short notice at great expense, as opposed to risking the caprice of acute emergency-based surgical intervention locally. —— Portugal’s median age, 46, is 5 years higher than UK and USA due to a markedly high baby boom 1960-1985. Like many nations the health care system will be saddled, even more, with a very high proportion of seniors going forward. -
It’s not uncommon and there is a literature on it that you can search. I assume you have had a positive SARS-CoV test, or signature COVID symptoms at some point, and that is the basis of your assumption for your own sleep disturbance. Bear in mind that test-negative research suggests that many folks pursuing formal testing for SARS-CoV-2 based on symptoms alone have unrelated illness. Therefore, a self-admin rapid test or lab test would have been your best bet, not simply illness symptoms. The probability to date of NOT having infection-induced seroprevalence as represented by nucleocapsid antibodies, in contrast to spike protein antibodies that result from EITHER infection OR vaccination, is approximately ‘snake eyes’ on a single die roll. In fact older persons are less likely to have acquired infection that in turn spurs natural immunity. The research on infection-based antibody seroprevalence is quite sophisticated and accounts for waning levels of nucleocapsid antibodies. If you have not had COVID infection confirmed, ie, there is some doubt you acquired it, and given the ratio of infection and non-infection history in the population, I would suggest ponying up some cash for a blood draw to assess for nucleocapsid antibody presence, often termed N antibodies by various labs. I’ve done it several times myself. I use Dynacare but my US contacts utilize Labcorp for the most part. To me, it would be worth it to confirm the basis of sleep changes in the absence of a previous formal infection disgnosis.
-
And you provided an essential early lesson with which he drove off, it is hoped and is likely, certified.
-
Kryptvaxon? Will it make my gassiness odourless?
-
For those 18-54 with exclusively mRNA vaxx history but interested in changing things up with the main established protein subunit option there may still be openings in this Novavax trial. https://www.clinicaltrials.gov/study/NCT05975060?cond=Covid19&term=Novavax&page=2&rank=11
-
The guidance indicates 6 months. See the last bullet point in ‘what you need to know’. That said, you probably won’t run up against much resistance if you pursue the new formulation earlier, particularly since the new variant seems distinctive and there is no evidence of harm with premature uptake. (USA FDA has set eligibility with merely a 2-month gap from more recent dose.) https://www.canada.ca/content/dam/phac-aspc/documents/services/publications/vaccines-immunization/national-advisory-committee-immunization-summary-supplemental-statement-september-12-2023-addendum-guidance-use-covid-19-vaccines-fall/summary.pdf
-
Entering haiku territory.
-
The ticket order site seems functional, so maybe it bumped out the main site? And Instagram is operational. https://www.redeyetickets.com
-
With that plunging, yes, sedation please …
-
Not yet rolled out here and “COVID-23” recently beat it to the punch, a virtual KO, fever 102-103F a few days; weeks to recoup health. Some 40 months was a lengthy period of time to be spared. One less jab this Fall. Though case incidence seems paltry compared to historical peaks, even correcting for ascertainment bias, one might lay low considering access is nigh.
-
A second go would require … TROLLS WORLD TOUR | Pinky Promise - GIPHY Clips GIPHY.COM The power of a pinky promise. 😱😱😱 #TrollsWorldTour in theaters everywhere April 17!
-
Oops, gonna have to wash it again.
-
Important announcement about Stock bar
+ SirBillybob replied to Dj Anthony's topic in Male Strip Clubs
It caught and convicted the sentence is $40 dances. Big deterrent. FullSizeRender.MOV -
Important announcement about Stock bar
+ SirBillybob replied to Dj Anthony's topic in Male Strip Clubs
It’s a challenge to be always ‘on’ too.
-
Important announcement about Stock bar
+ SirBillybob replied to Dj Anthony's topic in Male Strip Clubs
Correct. -
I tuned in out of curiosity when I saw that Marsden is Emmy-nominated. I found many of the hi-jinks to be guilty of being laugh-out-loud funny.
-
Not to mention that the judicious use of straps in both gym and dungeon should be elective.