SirBillybob
-
Posts
3,825 -
Joined
-
Last visited
Content Type
Forums
Donations
News
Events
Gallery
Everything posted by SirBillybob
-
According to his professional peers, Ally McBeal as well as power couple Lucious and Cookie Lyon he is the real deal.
-

Will doxyPEP create antibiotic resistant STDs?
+ SirBillybob replied to marylander1940's topic in Men's Health
Ongoing Doxy for bacterial STI research is sparse but, understandably, placebo control is now off the table. Results a few more years out. Without placebo arms, these are essentially superiority comparator research models though the working hypotheses are deemed non-inferiority comparison as the framing of ‘just as good, or no less ineffective’ is preferred to ‘better or less than’. Gunning for evidence of superiority also tends to introduce methodological bias. If I refer to non-inferiority again and get whining from the rank and file about terms, I’ll merely suggest going upthread. Don’t join the seminar if you’re anaphylactic upon the call to a bit of heavy lifting. Obnoxious trolling minimally stimulates a sense of personal non-inferiority; I cannot guarantee that it’s not additionally evocative of an own troll goal. In Canada, comparing daily DoxyPrEP 100mg to DoxyPEP 200mg 12-24 hours post risk encounter (condomless oral or anal or both; insertive or receptive or both) but max 6 DoxyPEP doses weekly to control for the potential confounder of dosage-exceeding, aka antimicrobial overload, upon multiple encounters. Inclusion requires STI within past year. In Hong Kong, DoxyPEP 200mg 12-24 hrs post risk encounter, as in Canada study model above, but compared to on-demand DoxyPrEP 100mg using the same uptake structure (2-1-1-etc) as applied in on-demand HIV PrEP, in contrast to the daily DoxyPrEP (again, that version in the Canadian locations mirroring daily HIV PrEP). Qualifying behavioural STI acquisition risk past 12 months but not required to have had established an STI diagnosis within that frame. As HIV PrEP is often an accompaniment, those without encounter journaling, multiple juggling and pillbox management skills need not apply. Phew! Did I mention I just reupped my condom and tenofovir/embitritacine supply in keeping with my operating threshold situated on the dividing line between non-negative to negative about sex? -
He’s hot. I see him occasionally at one of the EconoFitness branches I attend. It’s a packed gym. He ranks about #22 in heat but it’s an extremely stacked field. Even then, #1 couldn’t get $1000 out of me because, well, brazen entitlement and poutine culture tends not to go hand in hand. But I could get with reasonable offers, without a doubt, some real lookers there. He has an interesting background, quite divergent from that which is locally predominant. Not my cup of tea, but that’s just me and it’s unrelated to his roots.
-
No I am not saying that. You said that, well some of it anyway. That was the springboard for my adding the shave and a haircut bits about ad deletion pre-empting the access into which you had tripped. Historical access by others is not the entry point; you did not assert that and I realize it was an inquiry addition that turns out to be irrelevant. The entry point is that the ad never made it into the vault and a search function will raise the ad’s presence outside of the vault’s entrance. A formal step must be undertaken by the advertiser to submit the ad to the platform vault in perpetuity where I assume historical cream-ation is supplanted by content cremation. —— No need to be self-effacing on a troll-saturated message board where it’s all-inclusively provided. Hugs. 😏
-
Many advertisers are not aware that expired profiles continue to leave track marks and that simply non-renewing does not expunge all components of the ad. I was surprised to recently see that a chap at my gym long gone from the biz, now married with children, had shown up in my own history via review function several years ago that I had no idea maintained a life on the revised platform. He was understandably appreciative of getting the heads up and that I had exercised the prerogative to redact my review; however, other reviews stood, along with his profile images that unambiguously denoted the profesh. He is now in the process of re-registering on a temp basis, as the webmaster has indicated that a profile can be entirely deleted upon formal request to the help desk, the rent . men platform version. I would not have known this except for just transferring this week from the .eu to the updated system where the witness protection program is on offer, assuming that was always an option of course. Anybody grousing about being denied a revisiting of a particular lad’s profile for concrete reaching out endeavours and offers to pad their offspring’s college fund may as well be aware that serendipitous access to such is an artefact of the naïveté of some providers falsely assuming their ad dropped off the planet’s face, in the context of likely majority intentionality for deletion. That may include Planet Romeo but leave that for another day.
-
The prize was inaugurated sometime past the passing of pasture who probly wouldn’t have needed to curry favour for it.
-
Or you could all just split the one spliff.
-
Did Rentmen change its layout?
+ SirBillybob replied to + WSPigBrooklyn's topic in Questions About Hiring
Well I learned something interesting. I don’t use the platform much. I had always used dot eu, at least since it emerged, rather than the newer dot men. However, I wanted to edit a review (positive feedback type) shortly following submitting said review due to a minor omission that I forgot to add. BTW, I always ask for permission to submit a review and knock on wood so far have had no reason to be displeased by an encounter that emanated from an ad platform. It was not mission critical but I reached out to the help desk out of curiosity and the team patched me thru to dot men. I was puzzled by the lack of an org, com, country code suffix but so be it. However, the dot men version was emphasized as superior and the review management function is only accessible on dot men, not dot eu. Lo and behold, I gained access to the aforementioned review. That said, the dot men version, unbeknownst to me and in contrast to the dot eu platform, seemed to contain a lengthy and cluttered history, going back years in fact including reviews of long retired providers, that I cleaned up just to get whatever content lacking utility out of the way. So, torn? Not yet. I guess it’s dot men going forward but I am an infrequent browser. I probably, compared to most, pay a greater fraction of platform fees compared to the composite of said fees and platform-sourced provider charges incurred by most other punters. I think that I have messaged no more than 5 advertisers so far this year that culminated in a few guys that landed into in-person meeting territory. I tend towards a shortlist-and-repeat consumer fidelity model and a very small contingent of chaps hitting a very decent regular payday. The majority of my hiring is not sourced from ad platforms. I also learned, to illustrate here my skill deficit, to block my viewing history that has in the past triggered a response such as: “hey I noticed you checked me out”. When I shop I’m open to security guards monitoring my moves but not keen on shopkeep hovering. -
"No Drama" and "Confidentiality Agreement" guys.
+ SirBillybob replied to viewing ownly's topic in Questions About Hiring
Signed: HothungXXXL Notarized by Flimflam Bamboozle & Associates I’m dying here. -
Will doxyPEP create antibiotic resistant STDs?
+ SirBillybob replied to marylander1940's topic in Men's Health
That of limitless limitations and the inevitable aggravation of unfiltered obnoxious townhall hecklers? But wait for it: your ballot will be shredded, unable to bear the weight of validation ticks coming your way. 😘 There could be XX chromosomes in the crowd. Will you be OK? Venues here and worldwide want to be sure to bend over backwards in accommodation but you’ll need to give advance notice. Help us to help you! I possess robust antimicrobial capacity for it. -
"No Drama" and "Confidentiality Agreement" guys.
+ SirBillybob replied to viewing ownly's topic in Questions About Hiring
Chuckling over this. The profile descriptors seem so constricted and boilerplate to me. It’s as if most providers plagiarize what they already see from others. The caveat of lack of desire for drama is too universal to warrant specification, as if a provider expressing the necessity of being spared drama believes that a subset of peers tolerates or seeks such aggravation. Pass. But that is far from my pet peeve. What gets my eyes rolling up into their orbital cavities is the superfluous descriptor “hot” that accompanies images or is embedded in pseudonym. There is absolutely no justification for attempting to lead the viewer to make such an assessment, as if ambivalence or reticence on the viewer’s part is open to influence by whatever wording the advertiser appends. (Well, I was hedging on whether those pics are appealing enough to me to run to the nearest ATM, but I’ll buy into it if you say so, … as if ambivalence about a photo of a main course eatery menu looks iffy but the server asserts: “Don’t get to wrapped up in the image; that offering is unimaginably delish and you should commit to overriding any ambivalence getting in your own way. Take it from me …” … “I agree the perfume bottle lacks the design finesse befitting the price-tag, Madame, but I can assure you that it has no obvious flatus notes”) You know who you are. And we already know you must be hot, hunbun,or why else would you be charging an arm leg tit and toenail for a basic life function. -
Thinking of hiring for the first time
+ SirBillybob replied to BlackSheep's topic in Questions About Hiring
In case you missed the slide on Human Papilloma Virus and it’s non-wimpy transmissibility nature including within lower-level vanilla-grade interaction, notwithstanding your viral subtype exposures already possibly on board to date, assuming your age puts you outside the window of younger persons’ vaccine uptake campaigns having been employed this century, it is strongly advised to seek and acquire a course of Gardasil9 vaccination. -
Thinking of hiring for the first time
+ SirBillybob replied to BlackSheep's topic in Questions About Hiring
A sheep could be rural. The question is does he have any wool and how many full bags can he exchange for the transient husbandry he seeks. However, as Mary emphasized with her little lamb, heed the clinical advice and dynamics in which you figure as but a complex transactional algorithm component including where humanism may be integral, but be wary of candy and provider recommendations from strangers. My biggest personal takeaway over decades: one story’s prince is another’s frog. -
Blink once and it could be one plot line, twice and could be another. Maybe nepo baby Kravitz didn’t clearly write in nepo-baby Hawke for a reason. Ambiguity ensued. He wears the perfume intended to wipe memory yet castigated by Slater for standing by when the females were victimized. All characters’ knowledge of enacted reality is transient. Yet he could be called out for paralytic inaction over which no recollection could be accessible other than that implied by Slater; how could he actually interpret that indictment? Can’t really. Yet you can’t blink at all or you’d miss why Slater had transient non-redaction of recall. The flower extract nullifies recall and snake venom from a random bite or that is curated as antidote to perfume reverses erasure. That’s the cartoon plot device that pushes the otherwise non-credible narrative along. Binary victim-perp categorization is confounded all round. At first glance it appears gender-stratified yet Stacy (Davis, a known face of #metoo anti-misogyny in real life) is perp adjacent and perfumed, and the old woman (the sole undrugged) is allied with Frida. Lucas may have been a token option for victimization but could have remained in a neutral zone according to whether he was a desirable for those cast as predatorial or whether he had a similar predilection for exploitive cruelty as most of the males. Similarly, it is unclear whether perps paid for the privilege or were all simply pawns of Slater and his Machiavellian shrink. Whoever saw dead people didn’t later. My take is that Lucas simply didn’t fit in due to mostly decent majority membership and most on the island had not been selected via vetting anyway. At the risk of plot-spoiling, Lucas’ outcome was unrelated to any particular intentionality of any type directed his way. In a consensual context I wouldn’t have particularly deemed him fuckable.
-
I would never need to fire a physician involved in my care … knock on wood so far … because I would have had the necessary and sufficient read on them within the first five minutes of interaction to determine buy-in that two ringmasters, each bringing their particular contributions, yields optimal co-existence in any health system circus.
-
Would that all writing were as consistent as frivolous whining.
-
The divide between pro- and anti- vax ideology narrows with the ongoing slow-walked progression of elaboration regarding the potential toxicities of mRNA vaccine platforms and their novel delivery systems. A quick search will reveal that these papers are emerging from reputable sources peer-reviewed in reputable periodicals, and not foaming at the mouth regarding the atrocities of arbitrary vaccine admin. While genuine adverse events have not been dismissed for obvious reasons not the least of which is that rapidly produced vaccination slashed back morbidity and mortality as far back as initial vaccine research in which SARS-CoV infection was equivalent in vaxx and placebo sub-cohorts, their type, breadth, and the occurrence ratios by administration are criticized by some clinicians as being well beyond conventional thresholds for which regulatory bodies withhold authorization on other products. Expansion of mRNA/LNPdelivery into other domains is sometimes met with early failure due to toxicity. That takes some of the shine off as well. The trend is that the naysaying regarding coronavirus vaccination remains based on some degree of evidentiary cherry-picking yet gradually departs from the realm of outright quackery. In this context, why would it be so unusual for a growing minority of physicians to question the validity of ongoing sequential (eg, seasonal) uptake? The vax skeptic crowd is getting more of what they need while devotees are prone to partial or complete turncoat rotation, are well over the honeymoon, cozying up to the protein subunit vaccine option that itself implies a ‘sommelier’ stance where the concept of toxicity evasion stands in for vintage preference, recognize the vast and growing quantity of mRNA individual or class action suits, or are getting behind the legitimate yet impractical suggestion that much more research be conducted on adverse event susceptibility factors that the Immunology field asserts is technically doable for eventually reducing primary and secondary mRNA platform adverse events by population denominator. Just go to another doctor? It’s likely that the next in line will promote the prevalent vaccine on hand. Nothing egregiously wrong with an overly simplistic suggestion in which a deleterious outcome specific to a single prophylaxis event is remote. The original physician is spared the anxiety of a possible clinical occurrence that remains quantifiably if not qualitatively less possible than the complication of coronavirus infection. His or her primary blunder was in not conceding legitimate uncertainty about the costs-benefits and not placing the decision conundrum squarely on the shoulders of the patient. That would be the reason for me to submit his/her walking papers. … Time flies. I just hit 8 seasons since my last SARS-CoV-2 vaccine dose.
-
Armchairs are always in style.
-
Much of what's told to public about health is medical dogma
+ SirBillybob replied to samhexum's topic in Men's Health
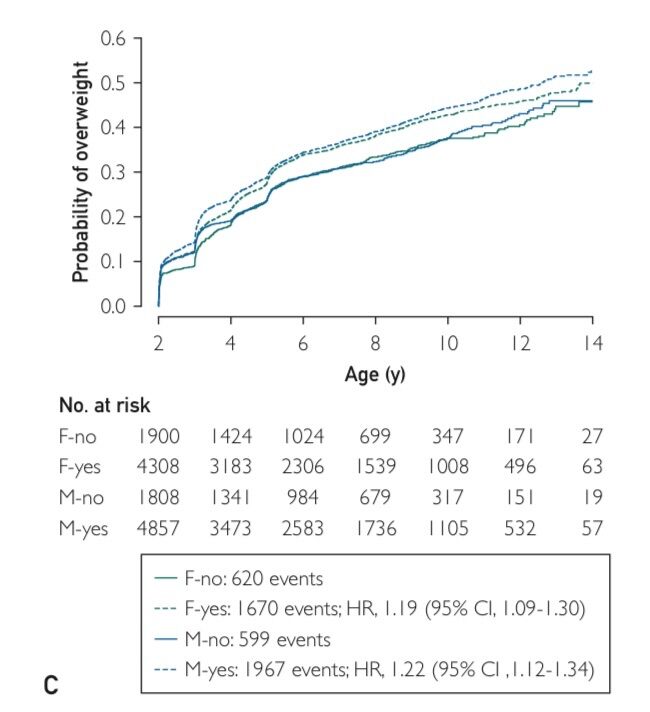
The good news about the Mayo study is that for parents promoting childhood obesity, early life antibiotic uptake does not significantly militate against the goal of having a population consisting of a majority of overweight offspring. The graph colours are inexplicably non-contrasting. With eye strain, the females are the slightly more green hue and males blue hue, hence boys a bit higher probability irrespective of antibiotic uptake. The broken lines represent early antibiotic uptake (binary yes-no not stratified for number of prescription courses) Many families override medical dogma, so there’s that.
-
I had merely indicated in a post (Aug 30) regarding the topic of who has ever had COVID that the assertion of having ever had COVID compared to the assertion of ever having had a cold was not the same considering there would be more additional time needed going forward to move the COVID dial from roughly 85% population lifetime incidence to closer to 100%. At that point the discussion would be moot, similar to the question of who has actually ever had the common cold. Your spontaneous response was that COVID for some people is worse in the long term compared to the common cold. While that is not untrue, I did not see the point of adding what is irrefutable but was unrelated to the discussion around assumptions of having ever had COVID. A shortfall of 10-15% of the population having yet been infected, that is escaped exposure, sheds no light on the clinical phenomenon of longstanding COVID health consequences, particularly as I add at the end here … Happy now? But I can see after a two-week hiatus that the thread has meandered all over the place. Surprising.😉 … By the way, there are several reviews on “long COVID” that put its prevalence from 5% to 50%. They are termed meta-analysis reviews because they merge several actual surveillance studies in combination. In spite of meta-analyses being of higher scientific standard, it is obvious that consensus on what it is and how many have it is sorely lacking. COVID conveniently explains the inexplicable in deteriorating health that could be, usually is, attributable to the less than fully explicable yet naturalistic. I will soon have a nuclear test for new onset cardiac symptoms. In 2019 I would never have mused about whether such symptoms were related to (confirmed) viral exposure or vaccination. Now who can help it, it’s all so front of mind. I am retired but there are likely a lot of folks unhappy with their employment that pursue secondary gain simply by presenting or believing in a clinical syndrome about which relatively little is known or agreed upon. It’s a bonanza for those that missed out on chronic fatigue syndrome because there is, in contrast, a true CoV pathogen and a remedy that mimics the pathogen. Hello disability claim, bye occupational drudgery.
-
The Canadian delay is administrative, not regulatory. NACI underscored importance of timely adjudication this year due to unnecessary cases last year as a result of late rollout. There is no clinical reason for PHAC to lag on approval. They insist all old formulations be destroyed first due to drug identification numbers common coding and some provinces’ pharmacies refuse to go weeks with zero stock. A “top doc” said a few people will get sick due to the delay but it is a small minority. Smells like a stalemate. Also lack of clinical agreement on integrating products for respiratory illness season versus getting a jump on COVID that seems first out the gate re: incidence seasonally. It’s a cluster fcuk. It appears that they could clinically approve right now but don’t want to be criticized for delay in dose administration because organizing staffing and appointments etc means additional weeks. And then the same for flu, and so on. They are holding out for concomitant dosing various diseases and dicking around with the hope that one or more vaccines will be in the same syringe eventually. This year the USA FDA got it right. I will likely get a ride to Plattsburgh soon and pay for a shot. But then I am born in Canada and pay for most of my health care out of pocket including testing, MRIs, colonoscopy, lab work etc, because my province permits physicians to bill privately.
-
If you had read me correctly you would realize that I was referring to the relevance of CoV pandemic incidence compared to the epidemiology of common cold incidence. 85% nucleocapsid seroconversion versus 100% cold occurrence (assuming most have had a lifetime cold virus) on a lifetime basis is not a morbidity comparison. By now, everybody is aware that COVID sequelae are unique.
-
Follow current vaccine guidance. Gone fishing.
-
Getting somewhere, maybe. It’s conceivable based on these metrics that many folks have accurately assessed their infection history. The basis of information for known yes/no infection incidence to date is based on lab measurable markers among subpopulations tested for those markers within immunity task force projects, eg blood donors, and extrapolated to genpop. Isolation is relative as its own state as well as in a context of other protective measures. It is one component of exposure risk. Pure chance is a major determinant. For a population single-infection history of 850,000 within one million persons over 4 years the estimate of 2-week contagion within interaction is 1%, 8500. You can estimate exposure risk from that. Non-exposure is 99%, as it is the pool from which infection could not occur. Over 4 years, a single-infection transmission potential from an infected person to a virus-free person is roughly 1%. Let’s assess the interaction exposure that yields a 15% chance of infection evasion. The number of unprotected single-event person interactions irrespective of closeness, intimacy level, etc, that nevertheless results in a 15% probability of non-exposure simply because infection and its transmission is impossible due to no pathogen present is approximately 189, minimally, a higher number in fact when accounting for one in seven persons within the total pool having not been capable of transmission because they never acquired infection. A lot of random or planned encounters could occur in Ozarks or wherever without incurring infection. That is why some of us were spared infection for a lengthy or total period of pandemic time while retired from lighthouse-keeping and canoodling with objects of affection.
-
At some point in the future the claim that most people from 2020 on caught SARS-CoV-2 will be an assertion more valid than currently. Perhaps the non-infected to date gap will close more rapidly if incidence patterns surge going forward. It will be as relevant as the question of how many folks have had a common cold.