SirBillybob
-
Posts
3,823 -
Joined
-
Last visited
Content Type
Forums
Donations
News
Events
Gallery
Everything posted by SirBillybob
-
I thought it was code for ankles in the assumed position in missionary work.
-
You guys. Leave this lad tf alone. By that I mean, sure, accommodate his unambiguous and circumscribed ask if you will, that consists of his modest little paper cash register for donations that you might supply while being circumspect about his context. He has wordsmithed his signage narrative just enough to legitimize requesting $ but falls short of asking to be rescued. He is not asking to be the face of any societal problem. 1 in 100 Canadian men are diagnosed with schizophrenia and the majority can “present” well. A higher proportion than 100% of general population have some form of illness within the realm of psychosis. If a cluster of men, however numbered, were to descend on him and convey knowledge of his background and he is mentally vulnerable his response may be no less predisposed to a triggered effect of paranoia than it might be coloured with appreciation of the crowdsourcing implicit in the well-intentioned story entered here. As has been suggested there is no lack of professional resources including street outreach services in the downtown Toronto district. I fail to understand assumptions you might have about the degree to which he is genuinely disenfranchised relative to the collective unhoused genpop, or what it is some of you think you can offer to make his connectivity to resources stick if indeed his plight is blockage to assistance access that you imagine you can transcend on his behalf. Good to be alert to the reality of those less fortunate. Perhaps a donation to Covenant House would satisfy the call to altruism.
-
 Slipped by us that charges were finally made: https://www.justice.gov/d9/2025-02/u.s._v._sikkema_indictment.pdf
Slipped by us that charges were finally made: https://www.justice.gov/d9/2025-02/u.s._v._sikkema_indictment.pdf -
Including 🎶“how much to do doggie with that endowed?🎵
-
This is not good for clients because of the implicit put-down that upsell amounts in the $100 range make us “cheapie”.
-
World-first gonorrhoea vaccine launched as infections soar!
+ SirBillybob replied to Danny-Darko's topic in Men's Health
Perhaps because our most recent vaxx dances have been with viruses. Viruses and bacteria have in common surface proteins, ie, antigens. The 4CMenB vaccine produces antibodies that can recognize and neutralize gonococcal antigens. Many of our routine childhood vaccinations confer prophylaxis against bacterial pathogens. My latest senior vaccine was for protection from bacterial pneumococcal disease. If I step on a rusty nail this summer my vaccine dose will not be virally based. -
I follow him as I do for many Brazilians but there’s no evidence on his social media of the Time Machine that has flung him forward to December, shaved off several age years, and reflects a continental shift or nuclear event in which Le Marais has landed in Picadilly. But he is in London currently. He last physique competed in 2023 and he is still in excellent shape. He hangs with another Carioca that I have met that similarly works the European circuit.
-
As Offred/June, played and directed by Moss in next to last Ep passionately put minutes before a viewer “WTF did that just happen!?” response, “Love Serena Joy; choose love.” Handmaid’s Tale.
-
Former Stock dancer Phillipe in serious trouble
+ SirBillybob replied to EZEtoGRU's topic in Male Strip Clubs
Haha. I don’t know what it is I don’t know but I’m sure it’s overwhelmingly vast. Like for example is T “the”, Theodore, Tiffanee (hommage to R Gere), or Twinkletoes? -
Tall, well-endowed, handsome, muscular hottie in Montreal - 411:
+ SirBillybob replied to Muscle Lover 2's topic in The Deli
D or double D athletic cup. -
Tall, well-endowed, handsome, muscular hottie in Montreal - 411:
+ SirBillybob replied to Muscle Lover 2's topic in The Deli
Well known several years as occasional dancer at Campus “Pepe” but he’s not my type and I don’t tend to scrutinize stage show or even private dance genital size. If I’m not planning private dances using a broader set of criteria I pretty much ignore the stage performance. Search Pepe platform wide for references to him on the local stripper scene. -
Former Stock dancer Phillipe in serious trouble
+ SirBillybob replied to EZEtoGRU's topic in Male Strip Clubs
July 9th, Longueuil criminal court division, a judge trial. I’m second guessing that May 15th was an adjournment with or without an appearance as the judge likely needed to formally review the defence representation aspect. -
When providers not truthful about size
+ SirBillybob replied to starman05's topic in Questions About Hiring
OK, height topic covered in depth. Width me or not? -
You probably already realize the probability is slim that a colleague will knock on your door without intrusive intent but for sociable or practical purposes, but the very fact of mentally downplaying the potential of something that would never otherwise migrate to front of mind could be the pea under the mattress stimulating a degree of hypervigilance that subverts the encounter. Since the work-based revelation risk component has entered into the discussion but is not a factor going forward in further hires I might consider paying extra to the guy this one time to book a room of his own there. This additionally makes it easier to extricate yourself in the albeit unlikely event you need an escape hatch simply because the match isn’t right. I don’t buy into the depth psychology framework that what may seem like a crack in practical damage control measures reflects a subliminal desire to emancipate self from a closet status that itself dictates the guardedness accompanying it.
-
A message from King Charles III: check your prostate!
+ SirBillybob replied to marylander1940's topic in Men's Health
I’m going to prevail on this for refuting my own senility, as I have picked up on the challenge of ambiguity posed by interpreting whether you mean that what slipped his mind was that doctors had informed him that he had been checked or that screening had yielded a cancer diagnosis. -
Montréal trip report (and first post)
+ SirBillybob replied to londonfunlad's topic in Male Strip Clubs
I would have no problem with any Montreal advertiser flaking on me. -
Is it standard for a provider to cum?
+ SirBillybob replied to cumconnoiseur's topic in Questions About Hiring
I assume that, like for most, while your own orgasm may yield the secondary benefit of being appreciated by another, the pathway to your own arousal that is sufficiently robust for orgasmic inevitability relies on more than that secondary benefit, particularly in solo self-pleasuring. Without the necessary true arousal occurring because of missing components at the time you can simply move on with impunity, wait for another day. It’s not another dollar that promotes the erotic aroused state, more than the basics of physical erection, you yourself rely on for orgasm. In fact, your own arousal will now rely on the inevitability that the orgasm you require as bottom line may also require that he convey to you in some way a convincing degree of arousal, appearing adequately similar to the sufficient natural aroused condition you yourself possess as leading to your own orgasm. Perhaps you could imagine hypothetical contexts for yourself where your access to your own orgasm is impeded by absence of some or all of the factors that heighten the arousal upon which subsequent orgasm depends. If you were to try to enact them you might risk enhancing the challenge of feeling convinced that your escort partner is genuinely aroused when you later transact. Not so much a problem if you can concede that his orgasm is performative and does not hinge on desire and arousal stages in the way that we naturally access such sequences to get to orgasm. However, you might also become more tuned into the dilemma posed by an expectation that the escort perform arousal and orgasm for the sake of an outcome that may deviate widely from what impels those phenomena more naturally in his non-transactional sexual experiences. Punter belief and assertion that the escort is genuinely turned on in a way that approaches his experiences based on preference is usually a suspension of reality. But then fantasy figures prominently so that’s OK. The important thing to consider is that metaphorically at least one if not both of you has his hand tied behind his back. What could be more natural than to desire that one’s partner is authentically turned on and that the authenticity could be guaranteed by a standard objective monetary reward? However what we want and think rigidly is essential may get in our way. You may also discover that simply conveying you really appreciate, without potentially deal-breaking insistence, an orgasm that he possibly but not inevitably will have accessed when with you won’t drastically reduce the worth of a collective of the hiring experiences over time. -
A message from King Charles III: check your prostate!
+ SirBillybob replied to marylander1940's topic in Men's Health
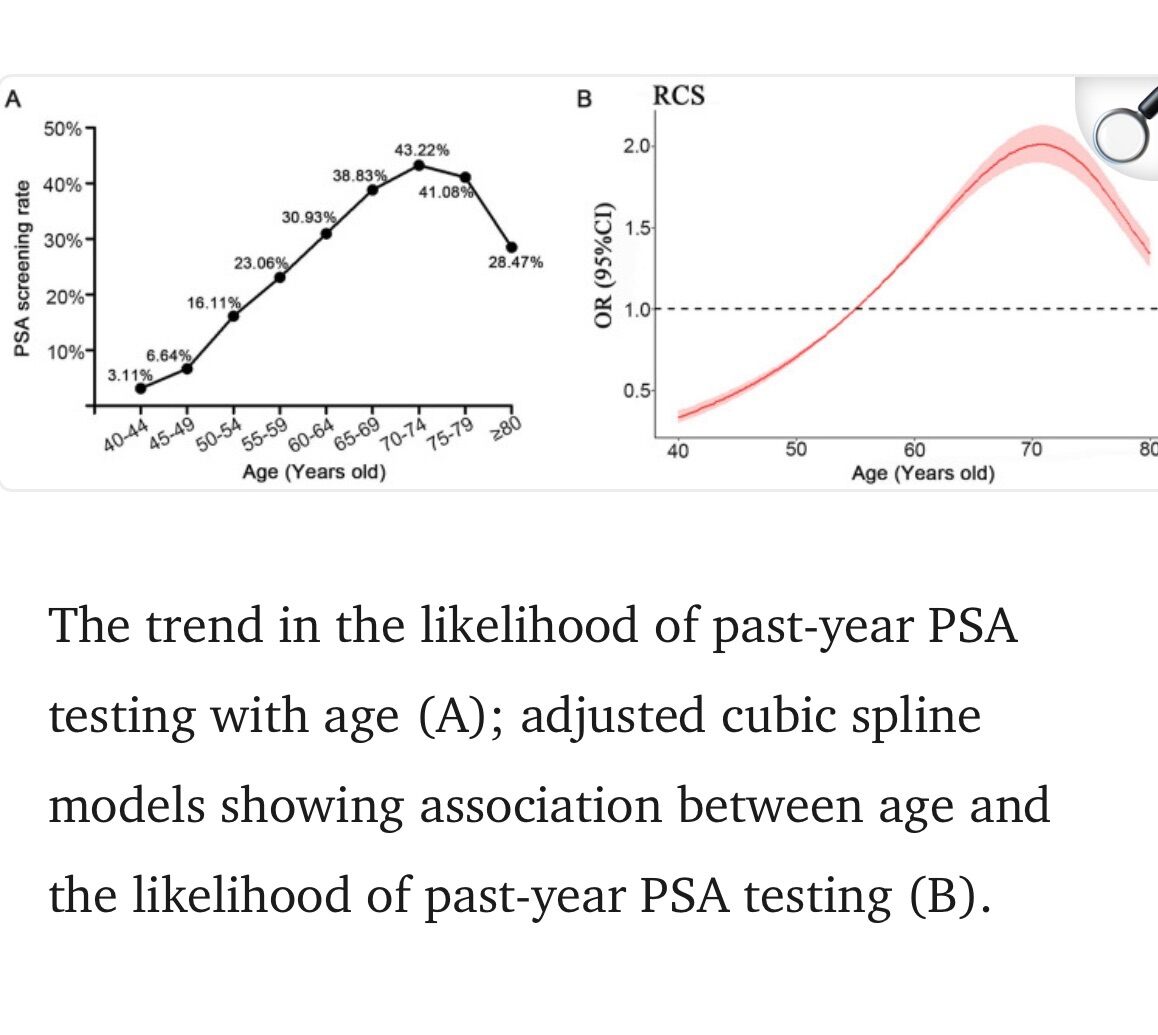
The rate of PSA testing uptake declines by age particularly from the point of age at which Biden reportedly had been last PSA screened. There are no data for 10 year iterations of testing uptake at any point in age, so it’s difficult to extrapolate uptake yes/no from data restricted to a calendar year, but the USA guidelines revised shortly following his test a decade ago recommended against routine screening for age >69. Annual testing rates that deviate from the guidance simply reflect discretionary testing, partially due to the transparency accompanying guidance that grades the recommendation for non-testing for the oldest of the three stratified age groups, as highly recommended in tandem with a low grade of evidence for legitimizing the non-screening, neither of the two grades moderate. The decline represented in the curve is obviously not related to increased mortality because all rate denominators are live males. It’s certainly within the realm of possibility that 10 years could elapse without repeating a test done around age 70. I don’t see the pressing need to speculate since several scenarios are possible and the overall picture for this disease and its variability would suggest that the pressing driver for establishing concrete from elusive is political backdrop as opposed to what is clinically expedient for management and the minuscule value of a single case for adding to best practices. For the highest age group the rate of prostate cancer of any grade is higher than the PSA screening rate that itself alone is non-confirmatory for cancer presence that is actually extremely common. It’s as if screening becomes oddly habituated according to historical testing uptake but yields minimal value.
-
A message from King Charles III: check your prostate!
+ SirBillybob replied to marylander1940's topic in Men's Health
Well, no. Inverse relationship Gleason score and time to metastasis so just a few years from onset of prostate cancer eventually graded as aggressive is not an outlier case. -
A message from King Charles III: check your prostate!
+ SirBillybob replied to marylander1940's topic in Men's Health
He evidently had a PSA test in his early 70s although screening guidelines for that age are in the ‘discretionary but not recommended’ category. Who knows what the results were although it’s very possible that there was nothing found in the result that prompted a prostate MRI or otherwise further investigation. It is also unclear as to whether the recent nodule that itself presumably prompted biopsy for confirmation of malignancy was detected via DRE, MRI, or both. The information rolling out is ambiguous though that is typical for media reporting outside of considerations of deliberate content distortion. The typical rush for first place finish on headlines consistently results in factual inaccuracy. The screening he had did not prevent eventual prostate cancer diagnosis whose new incidence is so common anyway at his current age. A large majority of octogenarians that die of any cause have prostate cancer of various grade that did not manifest or kill them before the non prostate coup de grâce that did the job. The average additional male life expectancy, non-adjusted for prostate cancer, is 5-7 years at his age and prostate cancer could be a co-factor added to his other health status vulnerabilities that shorten that added span. However, surveillance prevents very few prostate cancer deaths per 1,000 PSA-screened in spite of how ubiquitous prostate cancer is. PSA is a soft surrogate marker of cancer. He landed within the greater than 99% of males screened for whom such screening did not culminate in the detection required to mitigate morbidity and death due to prostate cancer occurring later, that large percentage of course encompassing collectives with or without eventual prostate cancer, even though far more than 1% of males will have such cancer within their lifetime. At least he is now accurately diagnosed and with no delay in timely best practices intervention, not subject to the problem of overdiagnosis of cancer that emerges with widespread screening and will have ultimately been of relatively innocuous grade or non-implicated in all-cause mortality, a phenomenon that figures prominently in (surprising to many) clinical guidelines that discourage routine PSA testing. -
Regent Park Community Health Center walkable from this lad’s piece of sidewalk has drop-in shower services and access to laundry equipment for the unhoused. I doubt that he is completed stranded.
-
World-first gonorrhoea vaccine launched as infections soar!
+ SirBillybob replied to Danny-Darko's topic in Men's Health
Further research is desperately needed. There is yet to occur a statistically significant prophylaxis effect within the gold standard methodology of randomized control trial. Differential effectiveness by anatomic site (urogenital, anal, pharyngeal) is unknown. Serological correlates of any true protection are yet to be identified. If you can qualify and spare the time for a trial that may be accessible geographically, and tolerate possible random assignment to placebo, you may be doing as much a worthwhile service as uptake of 2 vaccine doses alone. The tradeoff of infection due to non-vaxx control study arm assignment may be tolerable to you given the lack of impressive efficacy to date and the prospect of effective treatment upon infection in spite of growing antimicrobial resistance. ADDENDUM: Oops, apologies. No such ongoing or additional studies currently recruiting research subjects seem to exist. The small challenge trial in North Carolina where subjects are assigned to vaccine or not and then clinically infected with gonorrhea, obviously with treatment backup contingencies, is progressing at a snail’s pace with results still years out. Use, or supplement vaxx with, according to taste:
-
The downtown social assistance office is at 111 Wellesley St East which you will realize is actually within the gay village. Unhoused persons are typically eligible for $343 monthly for basic personal needs, as well as perhaps more importantly a zero-deductible provincial drug benefits enrolment for prescription medication and coverage for certain but limited dental emergency services. *** I would imagine he will already know about such programs.*** A person can acquire a slightly greater additional amount for housing costs, obviously a shared place or a rooming facility typically as dodgy as a formal shelter. The catch is that to qualify for the full albeit meagre assistance package the person must attend a program geared to training and progressing towards employment. They must also formally provide evidence that the housing amount is being used for such purposes. These criteria pose an impediment to many unfortunate souls who may find it preferable to take their chances as unhoused while prevailing upon passersby for informal substitute assistance or such assistance to augment the aforementioned basic needs government amount that itself requires some degree of jumping through hoops. If you ask him about possible current receipt of such funds, in order to screen for implementing a plan of facilitating government aid, that may paradoxically discomfit him because the premise of public-facing importuning for aid is the assumption of 100% destitution. I suggest a pleasant acknowledgement of his existence, token donation, and moving on. You may hang briefly quietly but if he doesn’t initiate his side of conversation yet politely responds to your chat I would take that as he can leave it. His street activity is his job, however sad and by default it seems, so don’t crowd and cramp his place of employment or expect him to sing for his supper by accommodating your well-intentioned desire to help. The Timmy’s cup defines the desired aid: cash, not java or a hotel key card. The sign delineates thanks in advance.
-
Not really. However, Mon Aug 4th this year is an official statutory civic holiday in most of Canada but Quebec supplants it with St Jean Baptiste Day in later June. Nevertheless, the 1st Monday in August tends to be taken unofficially in Quebec by many folks to add a summer long weekend within the stretch from July 1st to Labour Day weekend, or other Canadians come here.
-
Outrageous donations for the company of providers
+ SirBillybob replied to MCR's topic in Questions About Hiring
Maybe, but not to be confused with the perhaps larger quantity of bilious airs.