SirBillybob
-
Posts
3,822 -
Joined
-
Last visited
Content Type
Forums
Donations
News
Events
Gallery
Everything posted by SirBillybob
-
The form is designed poorly. If Bisexual is the third answer option then it should be called Straighty-Gaybe unless the other two options are stated as Heterosexual, Homosexual.
-

Question for the forum re copyright
+ SirBillybob replied to + Twinkluvr's topic in Questions About Hiring
These taste artificially chemical. 503 - Service Unavailable Error WWW.AMAZON.CA -
Question for the forum re copyright
+ SirBillybob replied to + Twinkluvr's topic in Questions About Hiring
Copyright is predicated on original, usually creative or invention, etc, work. Most things put out there in the public domain do not fall under copyright. That the author, poster, etc within social media or business platforms says it’s under strict copyright is an empty assertion, etiquette framed as imperative. The advertiser would not have objected to positive commentary associated with his linked ad. The complaint is his assertion of misrepresentation of his person and work and this leans towards defamation, not breech of image ownership. That he may view it as libellous is unrelated to copyright. Think of reviews of restaurants, hotels on Tripadviser. He should be grateful that Rentmen is set up to skew ratings for its own profit margins but not that he is spared the need to critically appraise how he might improve his services. -
How long does it take PreP to work for Tops?
+ SirBillybob replied to Constantine's topic in Men's Health
Yes, for zero risk to override relative risk, one oriented to risk elimination and the other to risk reduction. Risk elimination nullifies the concept of difference in need or requirement, and there’s no call to triage, because as you suggest one spark is the necessary and sufficient condition for infection. In that sense need is absolute. Need is not always absolute in retrospect. There are far more situations of non-infection resulting from unprotected sexual intercourse with a partner with unsuppressed viral load than situations of infection culminating from same. The guidance target is risk elimination and errs on the side of caution, but the statistical analysis reports risk reduction. 100% protection, say, no poz sexual partners, also renders the position risk difference moot. Otherwise, protection is on a gradient and condoms are recommended to supplement PrEP. Injection drug users need the same degree of protection as anybody to prevent HIV but cannot acquire enough through PrEP. We know that for sure but not for sure whether bottoms on PrEP are more likely to be infected. We push condom supplementation without making the distinction between top and bottom because the bottom cannot be protected without the top protected. Symbiosis. It’s the same intervention although logically a bottom on PrEP is more likely to be infected because pre-PrEP the risk difference is clinically significant. The condom intervention is applied differently, a difference in the life trajectory of the product necessitating negotiation, unlike for PrEP if uptake is uniform. PEP would be offered equally to a top and bottom, all else equal. They need the same degree of post-exposure intervention to escape seroconversion. If they asked about risk without the PEP uptake it would be a disservice to withhold the estimated difference while at the same time you push equal access. You might be more worried about a bottom taking a pass on the intervention. A top discontinuing PEP at 3 weeks might be less worrisome than the bottom doing so. But there’s no reason to adjust the resources as you might for different sizes of fire. This isn’t to say that PrEP resources aren’t ever allocated according to risk difference since females have 2-fold risk. The need is the same because sex is symbiotic. -
How long does it take PreP to work for Tops?
+ SirBillybob replied to Constantine's topic in Men's Health
Well not exactly, in purist inferential statistics terms. The metric of efficacy when stratifying the two risk categories is unknown for each separately because, as you say, the risk probability differs. Research evaluating PrEP effectiveness, that is, percentage of infections prevented that would occur without the intervention, would need to compare tops with tops or bottoms with bottoms. That won’t happen as it was always going to be logistically impossible and is now unethical given prevention is incontrovertible. Furthermore, a position risk distinction is not made and the categories are combined when the pharmacokinetics of time to drug concentrations correlated with protection are studied. Like I’ve suggested, in the context of not establishing whether PrEP is more effective for one versus the other position it’s best to treat them the same as opposed to implying that gaming the risk variables is valid and safe. -
Bitt chew kann.
-
How long does it take PreP to work for Tops?
+ SirBillybob replied to Constantine's topic in Men's Health
Right, negative event (target) probability is key. Drug concentration is on a gradient. Some is better than none, yet inferior to the estimated ideal. At any degree of drug concentration the intent for the bottom is that not one ball representing the target be pulled from the bingo bin. The intent for the top is that not one ball representing the target in a collective of 12 bingo bins be pulled from any of the dozen bins. The risk for the non-PrEP top approaches the risk of the optimal PrEP bottom. The risk cannot be the same based on position alone. It depends on number of encounters. Because number of anticipated encounters isn’t considered in the estimate of efficacy it makes sense for both tops and bottoms to pursue optimal drug concentrations for prophylaxis. Like many things, the answer is “It depends”, but the simplest answer is for all sexual positions to acquire the benefit from the pharmacodynamics research that governs best practices. Added to this is the notion that event risk does not reset to the same probability following each successive avoidance of the negative target. The probability of the event avoidance must be subject to an exponent representing the cumulative number of occasions in which the negative event is potentiated. All things equal, each successive encounter poses greater risk even if negative event escape accrues. My hundreds of unprotected sexual encounters between 1981 and 1985 mean I am at greater risk for HIV infection now compared to today’s chap on his first or tenth encounter, what have you, all other factors equal. Nothing to do with age or wear & tear. When it comes to probability, a debt in one way or the other is always owed at the multiple threshold. -
Don’t know but I think that there could be a chapter on taking a silly consensus-resistant topic to a progressively ludicrous level for fun.
-
Butt jist tuh fist bays. Better hee mite slyde inn att thurrd bae slayed dere. Datz neer inning homey ruin.

-
If Boston’s a true gay bottom he might be willing to pay $1,000 in Cali to my Brazilian $100 go-to situated in Rio. My favourite for a decade due to appeal and attitude, not price. Getting, being and lodging there is the $ kicker. I’d subsidize it by $500, a discount in Boston’s favour for the Boston creampie, to watch even just for the sake of a bucket list checkmark.
-
Bogotá, Colombia (December 2022/January 2023)
+ SirBillybob replied to + José Soplanucas's topic in The Americas
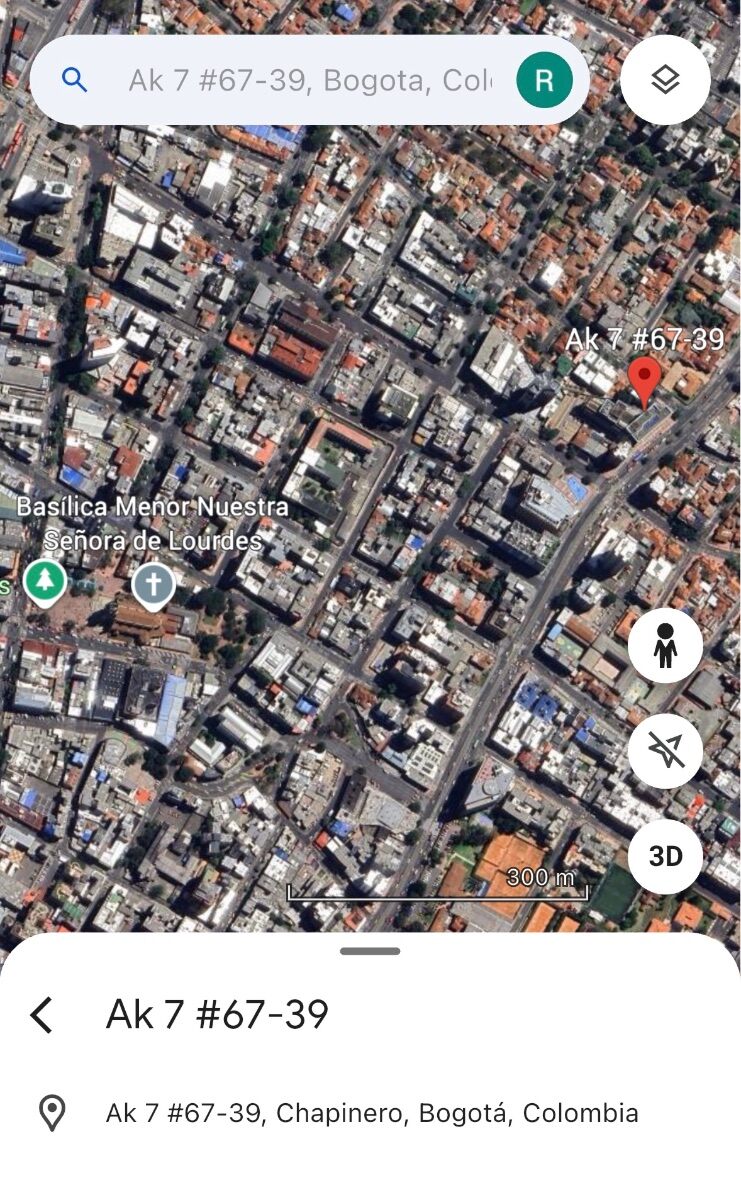
I have consistently stayed in Chapinero because it is accessible to all sights but also happens to be walkable to my preferred playbook of trade, St Moritz baths/brothel and vast eating options on the route as well as upscale groceries and walkable love hotels for hook-ups. The facilities for play at St Moritz are dreadful. I discovered that the north west facing side of the Holiday Inn at Carrera 7 & Calle 69 is quiet because otherwise the traffic can be quite noisy for sleeping facing Carrera 7 and other accommodations may be noisy for the same reason. It also has the essential mini fridge and microwave. Airbnbs east of 7 (or west for more selection) in the Calle 60’s may also be a good option. I booked a fantastic penthouse a few years ago with a stunning east view of the hills but it’s now off the platform. I liked Holiday Inn for the familiarity of the area but would in future return to Airbnb options, though actually I’m over Bogotá due to having max’d out the platonic side of my love affair with the city. For trade, Brazil wins, no contest when levelling nonsexual aspects of destination appeal.
-
Is it really all hell breaking loose, though? There’s no Groundhog Day -grade commentary on auto forums and the themes there don’t intersect libido and cash. All that’s being opined is that at a certain point any discussion of objective price and subjective worth is superfluous and gratuitous when it would necessitate a shaking off of criticism and devaluation whether or not the object of criticism were to be exposed to same. Moreover, a savvy advertiser is cognizant of the reality that such critique arises from a dismissible irrelevant few. It’s client yield that influences price. The topic may be unstoppable but tired and boring enough to align the brakes. ~ Herb
-
Au contraire, a leading question masquerading as a statement. It implicitly offers safety in numbers regarding the judgement. The ad asks for a leap of faith because he is making one based on viewer screening. OP leap of faith is that others corroborate a view of ad audacity as filtered through one subjective perspective of appeal against price. A more neutral approach would be to simply inquire a 411. You’d have yielded the leading question through introducing a starting gate with answers to a question that was not actually posed.
-
Cleanly, then: “Oh. My. Goodness! Fiddle Dee Dee! Waaaaaah! Wowza! Ooooomph! Clean them pipes, Mister! Don’t stop! Aaaah! Clean them into next Tuesday!”
-
How long does it take PreP to work for Tops?
+ SirBillybob replied to Constantine's topic in Men's Health
I think he was asking whether there’s a relationship between sexual position and number of days of PrEP pre-loading to confer equivalent pharmacological protection among the categories within the sexual position variable. This is a complex question because anatomical sites vary according to infection susceptibility and the degrees of drug concentrations and time on drug required to shut down replicating virus within mucosal tissue. So technically, there’s a theoretical basis for assuming less risk based on insertive sexual position, given receptive anal is 10-fold riskier than insertive anal, that itself compensates for the sub-optimal drug concentrations associated with sexual activity prematurity undertaken within the arbitrary, ie, 7 day, preloading rule of thumb. But this is really getting into the weeds and the guidance wouldn’t be easily packaged or consumable with this level of stratification detail. The risk arising from deviating from the 7-day preloading guidance may be mitigated by an impromptu transition to the 2 of 2-1-1. In fact, some guidance entities are happy with getting into the weeds on logistical tailored bilateral transitioning options between the two conventional uptake models. That said, efficacy isn’t the exact term as efficacy is calculated statistically from research cohorts and comparing two or more samples not representative of any one unique sexual interaction. Condom use also occurs among PrEP research subjects and may make the key difference for breakthrough infections that would otherwise have occurred. Undocumented condom use is a behavioural factor that supports efficacy confidence intervals as much as does the imperative of acknowledging statistical power and conceding less than the absolute efficacy metric. The all-it-takes idea regarding that low virion quantity that escapes prophylaxis is relevant enough to structure the guidance equally across the sexual position categorical variable. Where PrEP is researched and position assessed there are relatively few tops that aren’t sides. If all or most were exclusive tops the research cohort would have to be increased to astronomical numbers in order to achieve adequate sample power for meaningful statistical analysis of efficacy. The greater the background incidence of the thing the intervention aims to prevent the greater the reliability of the effectiveness result. Paradoxically, though, the value of 100% is that it can never be. -
Rapunzelo, Rapunzelo, let down your earlobe hair.
-
How long does it take PreP to work for Tops?
+ SirBillybob replied to Constantine's topic in Men's Health
That and Quiet 2: Even if adherent a re-infection will likely elevate viral load to above the undetectable threshold if not above the virally suppressed threshold. You may be essentially having sex with one or more previous D=T partners and he won’t necessarily know his TasP and U=U are subverted with an up-blip in viral load, maybe even transient superinfection, in spite of having been taking meds properly. A condom in my wreckedom if you please. -
Trapped in a tower?
-
I’d be more than eager to embrace the following tradeoff: an increased number of escorts that screen out based on client looks for an equivalent increased quantity of escorts I would screen in based on looks.
-
Yeah thanks for the Saturday nite back bacon on bagel or burrito cravings, bae.
-
Firstly clean and oil your keyboard for optimal smooth typing.
-
Lauderdale Club Visit (Johnsons, LeBoy, Boardwalk)
+ SirBillybob replied to MrDakota's topic in Male Strip Clubs
OK, Tony, I’m in. It usually takes me 10 or more. -
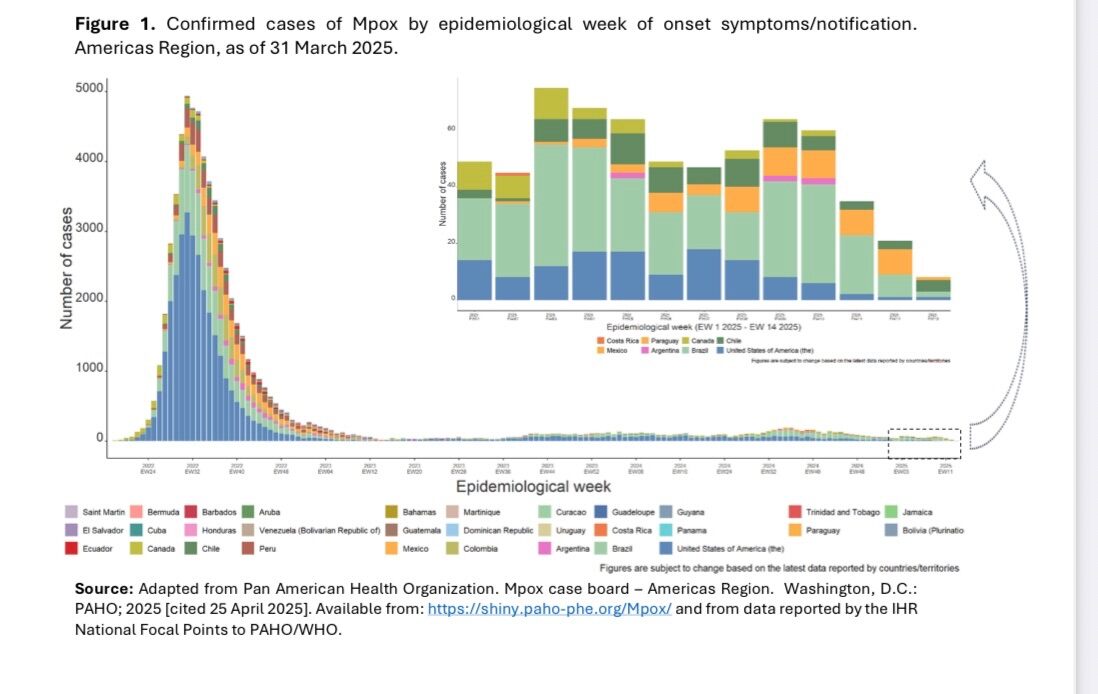
Here’s the link that enables views of Americas region trends less blurry than my screenshot. https://www.paho.org/sites/default/files/2025-05/sitrep-mpox-apr-2025.pdf
-
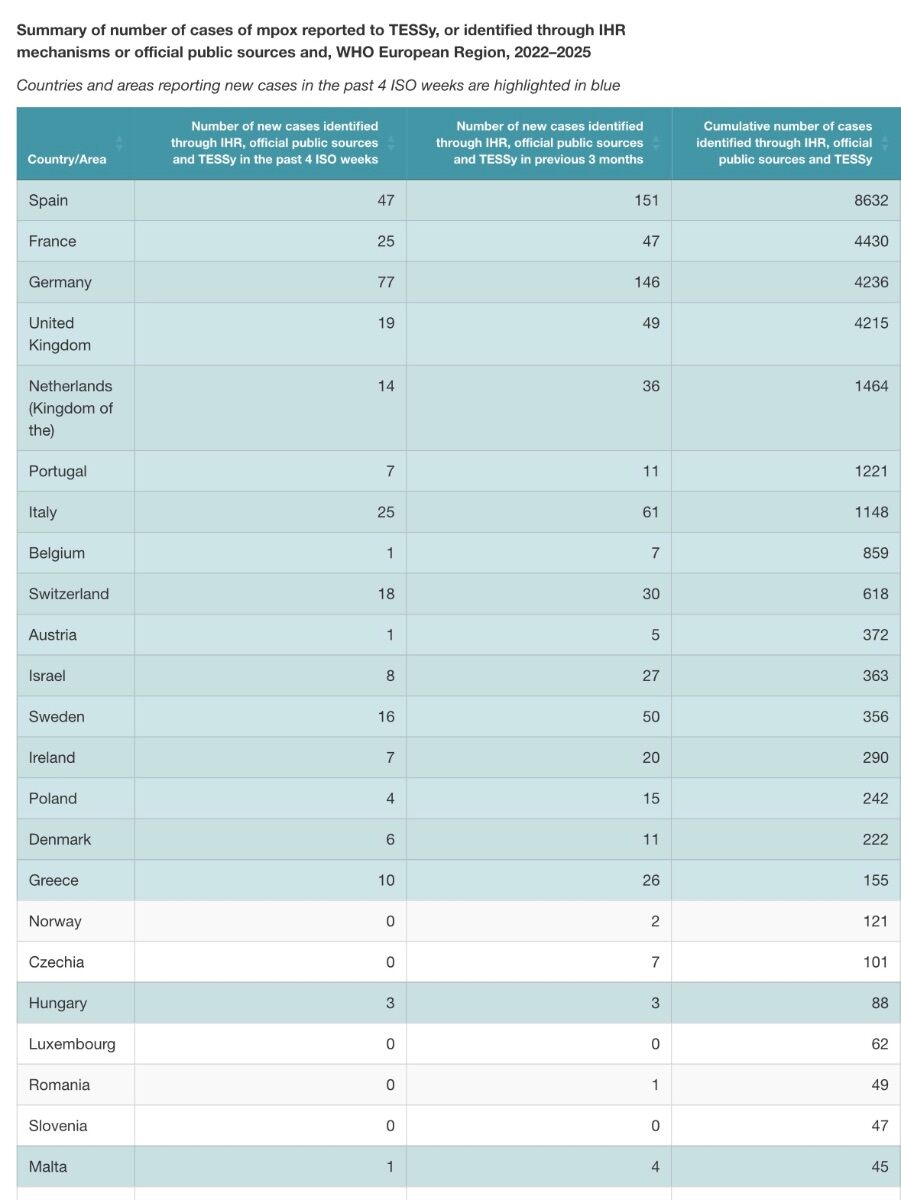
Use your judgement. Recent incidence trends are always available. Right now Spain, Germany, and Brazil appear highest risk and you can assess in the relativist context of peak rates, but nation-specific population denominators are absent in these metrics.
-
Time can fly on us. Are you sure 2 years ago and not when vaccine uptake peaked 3 years ago? In any case Canada’s national immunization guidance entity did not rule out booster doses of MVA-BN a year ago because of Mpox evolution trends at that time. However, just recently revised the guidance to state that a follow-up dose to the initial 2-dose series is not indicated at this time. In fact I took the 2nd dose last August because any time span between doses is permissible and I had been historically Smallpox vaccinated, as well as intending to escalate interaction 2024-25. However, you would be advised to pursue consultation about vaccine immediately if you have a suspected or known Mpox-infected contact, for post-exposure prophylaxis purposes, irrespective of your MVA-BN dosing in the context of the outbreak. As it’s often unclear it would be discretionary and depend on factors such as community incidence at the time. I doubt you would be denied if anxious following an occasion of intimacy. With trade I customarily inquire about vaccination because it makes sense when you are purchasing enjoyment accompanied by safety and offers an entry point for educating those at high risk yet poorly informed. What I do behaviourally, beyond PrEP to prevent HIV, and to mitigate STI potential crosses over to reduce Mpox transmission risk.