SirBillybob
-
Posts
3,823 -
Joined
-
Last visited
Content Type
Forums
Donations
News
Events
Gallery
Everything posted by SirBillybob
-
About a dozen cases reported to date. You cannot access MVA-BN there.
-
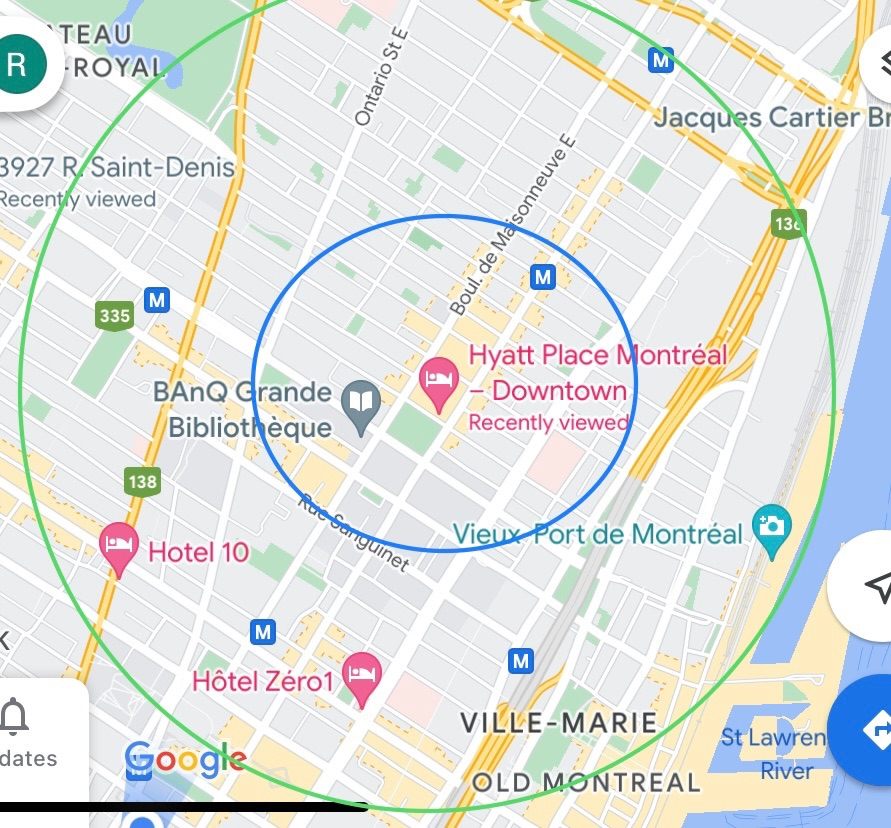
I drew a green circle representing the distance to Papineau Metro and Taboo. The inner blue circle is the distance to Beaudry Metro. A very popular restaurant in the city’s top-rated guides, Le Mousso, is at or near the blue circle, Ontario St. O-Thym near the hotel is not in Time Out’s top 50 but is fairly good. Many top restaurants reside within or very close to the area within the green circle, for me no more than 10-15 minute walk equivalency. If you would be fine walking a distance no greater than Papineau you would be within striking distance of a few great spots to dine. But you cannot just show up and you may need to book on an app such as Open Table. Singles do not fare well on busy nights in fine dining. You might want to seek a place, in that event, with bar seating that doubles as place setting. Le Bouillon Bilk is one such option, again, walkable right by St-Laurent Metro. Tiradito is outside the green circle but not by much; very good well-rated Japanese-Peruvian fusion and ample feeding at their bar if no table. This is not so much for you as it is for those less familiar. You yourself are able to find choice establishments while eye-candy drips off your arm. LOL

-
* in case seekers are coming to Montreal be aware the vaccination sites close early on 24 June and 1 July, 15:30
-
No, but you would register at the admin screening desk prior to the injection as Quebec residents, Canadians, everyone is required, with valid ID. Most in Quebec using QC health card, Canadians their province/terr health card or passport, foreign nationals their passport. You can see further instructions I have been posting in the Health section under ‘Monkeypox a new worry… ’ thread.
-
Sounds like $20, plus $80 sucker tax, unless he is trying to secure blocks of songs, ie, 5 in this case, that strategically makes sense to reduce number of contacts while earning. Strippers can get inoculated a block away. They should wait 2 weeks and be showing clients their Imvamune vaccination certificate. Their contact volume surely poses a greater risk to them, thus to you. And yes, the transmission risk for a lapdance in a tight area with physical contact and breathing inches away from each other is likely high, if either is currently infectious.
-
You’re right. The tenderness, redness, and swelling peaked Day 6-7 but has greatly reduced as of this morning (Day 8). ——— [For any reader] I am not well-versed in TikTok but when I scrolled back up in the thread to watch them again the presentations were other videos from ‘gay doctor’ … the platform just automatically sets to the previous or subsequent in a series? Oh, they reset. Never mind.
-
If ‘that gay doctor’ is one of merely 10 or so cases in Chicago, notwithstanding his occupational exposure risk (if that is the transmission vector; could be another) what a fluke. It suggests this virus is vastly more widespread than officially reported.
-
Technically it’s right on the side of the boundary street St-Hubert that puts it in the Gay Village, but it connects underground to Berri-UQAM Metro considered the eastern perimeter of Montreal’s Downtown or business district. Close call for Hyatt Corporate. 😏🤔 Considering the proliferation of drug trade in the area, it would risk being dubbed ‘High at the Gay Village’. Being situated in Ville-Marie borough, aka ‘Mary Town’, hardly helps. 🤣
- 14 replies
-
- 2
-

-

-
- montreal
- hotel gouverneur
- (and 2 more)
-

Stocks and the marketplace
+ SirBillybob replied to cany10011's topic in Personal Finance & Investing
I ill-advisedly tossed the die and cashed out a chunk of registered mutual funds at around the market nadir in March 2020, didn’t die, and I had planned to spend a lot of it but I haven’t needed to touch it as my regular income flow has been adequate even for 5 major trips I will have done and dusted this year. My fund manager asserted over two years ago that it would be a challenge to ever get that money back into the market. Now with the funds I left invested tumbling, I am wondering if the adage ‘never say never’ applies. -
I know all this, and that single-dose vial playbook further mitigates contaminant risk. What I did not add was that the nurse giving me the dose was really rushing and abrupt, though she had several minutes between recipients. She put the needle in seemingly outside the zone she had swabbed, not giving it more than 3 seconds to dry yet missing the target spot at that, and in a weird location on my lower tricep quite distal from my deltoid and my bicep boundary. (I have no tattoos.) Frankly, I am relieved because she did not put on a bandaid though everybody else got one, apparently plunked on their deltoid, and I wasn’t sure she had even correctly applied the dose, and wondered if I did not get a bandaid because of a mishap as opposed to there simply being no🩸 in my case to stain my light-coloured shirt. I don’t think the exact location matters much. I also know that alcohol prep is not essential and I had showered that morning. But the latency of this reaction combined with my dissatisfaction with the administrator had me second-guessing. My local redness and swelling with CoV vaxx emerged much more quickly. With the Imvamune it was slightly tender and now visibly much more swollen and red but only after 6 days, about an inch or more away from where I think the puncture was. I know I know … subcutaneous, therefore slower systemic absorption? I agree probably (or certainly) not cellulitis but, rather, thankfully, evidence of getting all the active pharmaceutical ingredients essentially in the right place.
-
Two leads to data, @Unicorn : The National Advisory Committee on Immunization I attached already. As is typical, they summarize and reference the related scientific inquiry. And/or the global database of registered studies Clinicaltrials.gov … put in Smallpox as the disease as it should bring up the very few Monkeypox-specific. Though taxonomy name changes are in the works such as SimianPox, hMPX & perhaps attendant clades. For the key word in the next dialogue box you can enter the overarching company product proprietary name MVP-BN (which I think is the generic name) that covers the trade names Jynneos, Imvamune, and Imnavex, or any one of those. There is one maybe two Jynneos, but others USA and beyond for MVP-BN, even some beyond orthopox specificity. Some of these studies/trials have results that link to published manuscripts on PubMed or elsewhere. You would select ‘all studies’ for the full breadth, ‘recruiting or not yet’ more for leads on being a volunteer. And as you likely know, stratifiable by nation. There is likely a small window to get Jynneos in Omaha or Columbus in a trial far more complex than simply MVA-BN immunogenicity on its own, but IMO probably easier to get Imvamune in Montreal.
-
There is no warning on the Quebec flyer viz immunocompetent versus immunocompromised because it is not contraindicated as such. In fact, the guidelines seem to prioritize immunosuppressed. Moreover, selecting and importing all of the relevant details from 25 pages of guidance does not fly well on a flyer, eg, stratifying by Simian Pox PEP versus PrEP intentionality, specific populations, Smallpox vaxx history, etc. However, dosing considerations, ie, single dose versus prime-boost/28+daysInterval may be relevant in terms of that aspect as well as smallpox vaccination history, and labwork-specific occupational risk factors for which regular boosters are recommended. The just released Canadian guidelines are national and eligibility is narrowly defined, but provinces have the prerogative to broaden eligibility based on community prevalence. Therefore Quebec has an open-door policy and, in fact, out of province or foreign nationals visiting Montreal etc may access the vaccine. In fact, the cis-/trans-MSM criterion is not rigidly applied and obviously immunosuppressed females can access it, though it has been available in Canada for a few years and medical specialty programs can dispense it as well. But based on my time observing at the walk-in site my sense is that absolutely any worried adult could get the vaccine. For example, younger parents that missed the standard Smallpox vaccination that ceased around 1972, their children similarly unprotected. Orthopox viruses are not truly eradicated. It remains to be seen what inoculation campaigns will re-emerge. Bear in mind your categorization for one versus two (even 2 plus later booster) doses. My sense is one is better than none if you cannot come back as a person for whom 2 doses is indicated, but that is obviously not my call. The national guidelines came out just after I was instructed at prime dose to return in 4 weeks for the follow-up dose. I will just stick to the single dose due to Smallpox childhood vaccination. This I put together from reading; it is early in the rollout game, info kinks to be ironed out, and I am certain the 2nd dose would not be withheld and that the frontline staff may be following provincial directives and not so much up to speed on the recent national guidance or working out the apparent contradictions. There is already some hinting in some of the literature that 28 days is arbitrary based on the limited extant research, not surprising given moving temporal dosing targets that evolved for SARS-CoV-2. For now, I feel protected. The injection is subcutaneous and I have latent swelling tenderness redness that seems to be suddenly pooling the most at 6-7 days post injection. It is likely solicited site reaction that will attenuate and not the rarer bacterial cellulitis (fingers crossed). Attached is the Canadian immunization guidance … https://www.canada.ca/content/dam/phac-aspc/documents/services/immunization/national-advisory-committee-on-immunization-naci/guidance-imvamune-monkeypox/guidance-imvamune-monkeypox-en.pdf
-
I went into the lobby yesterday morning. They weren’t too keen on people just coming in to snoop around as there were contractors making finishing touches for the soft opening that afternoon. The lobby is about 95% done. The fitness centre and pool are ready. I did not view them. The pool is indoors but apparently has natural lighting from windows. The name on the entrance door is Hyatt Place. It is a few feet from where the 747 express airport bus first-embarking/last-disembarking is now located n/w corner Ste-Catherine/St-Hubert. Here is one of many media articles on the inauguration: https://www.hospitalitynet.org/announcement/41008141/hyatt-place-montreal-downtown.html
- 14 replies
-
- 1
-
-
- montreal
- hotel gouverneur
- (and 2 more)
-
Right, me too, I noticed mine seems to have faded a lot. At the risk of stigmatizing it seems apparent to me that very light-skinned plump women have the most discernible mark, usually more indented than the BCG scarification that some folks possess. Other than that, there’s always wild goose-chasing reading articles that often fail to contain the one or two clues or answers one is pursuing. LOL
-
I don’t know anybody that had the multiple Vaccinia single-sitting punctures done over again in the exact same spot, or a second scar, so I don’t know what is meant by an apparent Smallpox booster apparently recorded in your certificate booklet. In Canada only lab workers involved in Smallpox research are advised to get a booster every 10 years due to unique exposure risks. I don’t know if it’s scarification in a new location each time, &c.
-
The fading of the scar is irrelevant. I also added an article to my previous post … we crossed in the ether.
-
Australia did not have mass campaign Smallpox vaccination like other parts of the world such as Canada and USA. That likely accounted for its necessity upon travel, even at a point at or close to global eradication, so you would not risk bringing it home where very few had/have immunity. As such, a non-contained global MPOXX pandemic would likely require prioritizing Australia for vaccination, since previous Vaccinia inoculation, that may crossover to confer some protection against MPOXX, was relatively rare. If you don’t have the pock scar you may received a later generation vaccine and booster; I’m not totally up on it outside of my generation in Canada. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7291091/pdf/viruses-12-00554.pdf
-
You would have the characteristic dime-sized Vaccinia scar on your upper arm due to bifurcated needle punctures, likely when in primary school. All other vaccines or boosters left no mark as were intramuscular or maybe some sub-cutaneous.
-
Canada has 350,000 doses stockpiled and a new much larger order won’t be available until 2023 because Bavarian Nordic in Denmark shut down operations to do renovations prior to this outbreak. Here’s the new guidance attached. I’m not summarizing it. The provinces/territories will need to decide their strategies as things move along. http://ow.ly/79n950JuVWl
-
I received an Imvamune (MVA-BN; Jynneos in USA) dose last week in Montreal (see flyer). It is cross-approved in Canada (PHAC) and USA (FDA) for both orthopox viruses: Smallpox & Monkeypox, and on its way for MPOXX-specific authorization, if not already this week, in UK and EU. They were not rigidly grilling seekers regarding the criteria, and did not seem to be turning anybody away, more interested in the teaching part than the recipient qualification aspect. They instructed to return for a boost dose in 4 weeks but I had read much of the scientific literature regarding those (eg, baby boomers) with a Vaccinia inoculation history and the prospects of immunity durability, thinking I would just go with the Imvamune prime dose. Then a day later that’s what NACI recommended irrespective of previous Smallpox inoculation. My sense is that that one rationale, muted due to the already quickly extant stigmatization, is the influx of 15,000 International AIDS Conference attendees in 5-6 weeks. The 2020 conference went virtual for obvious reasons and it would be a shame and tough on Montreal’s recovering economy should this one be precipitously cancelled as an in-person event. AFAIK Vaccinia-naïve PHA have always been prioritized for the MVA-BN vaccine against Smallpox, as an alternative to 1st and 2nd generation inoculation products, but this one must be approved for the Monkeypox indication wherever it is administered. Even if rolled out for Smallpox specifically (nudge nudge wink wink) with the off-label intentionality of Monkeypox prophylaxis, how to organize such a convoluted scenario for conference attendees broadly abroad. BTW, the disease may be renamed HMPXV (H for human) and clades appropriately numbered or lettered as opposed to geo-African.
-
First time ever, on Friday at Campus, noticed a female evidently getting a dance in the typical cluster of previously men-only private cubicles behind the DJ, as opposed to the cubicles behind the movable back-up bar curtain where I believe these typically took place for women on former Ladies Night Sundays. Also a customer with his hands groping his pet rodent face etc then shaking hands with others including dancers, as well as handling the slot machines. Zoonosis disease potential much? This would not have struck me prior to SARS-CoV-2 and Monkeypox here.
-
I’ll post this under Montreal strip clubs because it is where most Montreal content sits and a city search here will pull it up anyway: I recently planned to take this route west to the airport from Union/Frère-André which is just a few stops from the origin, that is apparently now StHubert/SteCatherineW a block west of the former launch/last-stop at Berri, but essentially the same block at Berri-UQAM Metro station. Perhaps due to the bike lane complication, etc on Berri. Twice a bus marked ‘en route’ or ‘in service’ (memory fails me) passed without pulling right to the sidewalk curb lane or stopping at around the expected sched times. It took me a while to figure out this was the 747 but without the designated route sign BECAUSE it had filled up near source and it only allowed as many passengers as actual seats. The sun was reflecting on the windows and I could not see the luggage rack as it was a few street lanes away. On the 3rd pass I got the last seat! after waiting about 70 minutes at the corner. I had given myself 4 hours and had priority check-in at the airport so was not freaking out. Therefore, to reach the airport I suggest taking this bus at the origin. Even then, perhaps a queue. The alternate route begins and ends at Lionel-Groulx Metro station but I don’t know how saturated the queue gets there boarding for the airport. In any event to get to either Metro station, you can use the same $10 scannable ticket. I also always carry $10 in one- and/or two- dollar coins in case the ticket fails to scan upon boarding the bus, as has happened once or twice over several years.
-
I don’t go to Taboo but I note that all the strip clubs are currently open to all genders all nights. At one of the clubs recently there were two young teenage girls blathering loudly behind the stool I was sitting on, taking forever to navigate the ATM machine. But we live in an inclusive society and one must adjust. Clubs also must survive and recoup where possible. I also noticed that Taboo put out an online questionnaire two months ago, presumably to acquire broader community output about activities. I suspect the unusual theme night is in response to that and will likely only be episodic, like the Violet Hour readings occasionally at Stock.
-
Agree. Underwhelming. I was at Mezzaninu a few years ago, about 3 visits so not entirely representative. Negotiated with 2 visiting go-go dancers, as no regular providers interested me. The city is pleasant enough for a few days. Trees were in bloom. There is a tree-canopied street listed in 10 top globally of that kind of thing. Bused to OK art museum. Flight was cheap. Stayed with an older retired professional couple in a luxe building. I think it was about $30. One might find a longer visit exploring Gramado, Canela, winery trail, etc all north of PA interesting. Those higher altitude regions actually sometimes get snow in July/Aug, a draw for Brazilians in more tripical/sub-tropical climes of the country. —— In COVID era, I don’t know. Likely not better, could be worse for trade.
-
Thanks for posting the link. As such, anybody here can read the full article Discussion and pick up that that the researchers are not dismissive of case-control methodolology that nevertheless downgrades it, relative to RCT, within the level of evidence hierarchy. In fact, many of the limitations are posed by the complexities of bias that affect that RTC gold standard for studies of this nature. Breadth of relative risk metric for the CoV component, albeit case-control methods, fleshes out the story. In spite of the elaborate cogent outline of limitations, a portion of which you selectively quoted, a large part of the Discussion strongly underscores the differential value of respirators in terms of infection risk receptivity. If you remove the CoV component, you are left with findings more reflective of the RCT grouping that were imported into the recommendation of respirators, in spite of no apparent effects for confirmed flu. Similarly, if you exclude confirmed flu, the remaining findings buttress the idea of respirator advantage, notwithstanding the research list’s minority proportion of non-RCT. This way of looking at the findings is analogous to meta-analytical data sensitivity analysis. A strongly persuasive totality of findings discounting respirator superiority did not emerge in this meta-analysis. One of the references is a meta-analysis exclusively RCT-inclusive and has a different angle, more summarily dismissive of a difference between surgical and respirator, yet presents limitations that undermine the evidence certainty. (See below) In sum, it would be easier to switch to surgical. I take all the input with a grain of salt, but a combination of behavioural habituation, and the limited extent of research findings in the direction polarized from where I think the balance rests, leaves me ‘team N95’. I am not suggesting absence of evidence is not evidence of absence. I did not intuit a preference. Rather, the evidentiary tilt at this point influences my choice. [Anyway, this is me OUT, off-grid this topic for now, heading to Spain with my travel declaration etc all completed, and better things ahead than a basically high-output low-impact board discussion such as this.] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7228345/