SirBillybob
-
Posts
3,823 -
Joined
-
Last visited
Content Type
Forums
Donations
News
Events
Gallery
Everything posted by SirBillybob
-
Key takeaway from BN elaborate preprint: 1st Imvamune dose is *booster dose post childhood Vaccinia (older subjects) & noninferior to 2 current doses for Vaccinia-naïve (ie, younger) even up to 2 yrs, but 2-year booster for the younger then supersedes older. The 2nd *booster for older seems superfluous for now; can defer to an undefined date. The question, then, is when should group older folks pursue uptake 2nd *booster in order to more closely equivalize the titres conferred by a booster at 2.5 years past primary series (6 months past booster for younger vaccinia-naïve), of course given unknowns about correlation between immunity parameters and protection. (Parenthetically, recent M&M Weekly Report suggests 14-fold infection incidence unvacc compared to single dose MVA-BN, and recommends 2nd primary series dose without stratifying according to Vaccinia history … likely the simplest guidance without creating confusion, ambiguity, etc, and no evidence of harm from a possibly essentially superfluous or premature 2nd dose application for smallpox vaxx’d) BN manuscript: https://www.medrxiv.org/content/10.1101/2022.09.07.22279689v1.full.pdf Caveat as always, often overlooked: immune response is predicated on Vaccinia and not specific to Monkepox: orthopox class transferability is theoretically imputed.
-
Canadian flu vaxx guidance is ASAP following product distribution and recognizes potential for Oct influenzidence uptick but the reality is that annual admin rollout usually lags into Nov and even Dec. In Quebec I used to have to scrounge for and pay for a shot at a travel clinic. Most GPs just won’t have or give it. They are too stretched and a huge swath of genpop has no GP, so it makes sense to task-spare. Most vaccines are now bookable on a web platform and available at many pharmacies. That said, pharmacies have only so much capacity to accommodate the full genpop. Some pharmacists give the jab; others book a nurse for a shift here and there in order to reduce the interruption of meds dispensing. It’s more organized now. It would have been shocking a few years back for a pharmacy to cold call phone and explain candidacy for Pneumovax or Prevnar but I recently received such a call. Canada had approved Moderna bivalent BA.1 and just a few days ago Pfizer BA.4/5, but pushing the former for now and dissuading genpop sommelier stance. But Imma hold out for Pfizer boost though last dose (Spikevax) 10 months ago. I want to rev ‘0 to 60’ from ancestral strain base to more predominant Omicron variant. The guidance for Luv2Play is 6 month boost interval but >3 months from his June dose is discretionary. As indicated, some of this hinges on how contrarian one’s critical appraisal of immunization guidance is. My exposure risk is low and I may have priority in the eventual Pfizer queue because on paper I have only had a primary mRNA series. In reality primed with an experimental protein subunit, a little piggy not making it market. MPXV vaxx (thread topic) thoughts to follow.
-

Covid vaccine increases death rates!
+ SirBillybob replied to Alex.Blessings's topic in Men's Health
I find this to be disingenuous. I began by critically appraising a Florida bulletin that derived from a lack of research acumen in interpreting cardiac mortality in terms of such clinical outcomes being attributable to vaccination. You opined that healthy people do not benefit from vaccination over and above infection, input unrelated to the thread and its hyperbole-slanted headline, and that the standard for assessing vaxx uptake legitimacy should be advanced awareness of one’s baseline medical status, notwithstanding the infrastructure impediments to that standard. That is simply unrealistic in the real world. Your viewpoint accompanied by a self-referential rendering of personal health status, related attention to it, and its influence on your own decision-making, as well as an anecdote about a gathering in which some transmission potential exists in spite of immunity and/or test neg’y, something we already know. Then you suggest that vaccination be a personal choice, seemingly predicated on your own distinctive advantage regarding health self-awareness, when in fact personal choice for a majority of decliners is confounded by distorted interpretations of science or rejections of compelling findings that support the merits of vaccination uptake. And you suggest that inferiority in health management self-efficacy is central to poor outcomes …. when the competing reality as we know it is that such limitations are not intrinsic to the individual. If you had opened with the Big Lie victimization and over-extrapolating from personal experience I’d have wasted less of my time. If you had begun a thread of your own I would likely have not responded. This is the liability of attempting to provide input into a topic. Lesson learned; the pandemic is one of convoluted thinking and tangential input. I am not in a position to disabuse others of their flawed views. In contrast, I was capable of deconstructing the data on which the misguided Florida public health guidance on vaccination was based. -
Covid vaccine increases death rates!
+ SirBillybob replied to Alex.Blessings's topic in Men's Health
Transmission, otherwise known as secondary attack rates, isn’t amenable to measurement because the assessment context is heterologous. All households contain a variable mix of immunity and its temporality. Household members also engage with the outside world. You cannot design transmission efficacy without a clear assignment of two separate scenarios held constant. Such a prospective design is cost-probibitive. This is one of the reasons that the basis of vaccination is oriented to morbidity and mortality. To suggest an elective uptake is outrageous considering that most people making that decision would be lacking comprehension of risk or are simply contrarian; they would not tend to be cavalier about the right to choose and its potentially dire consequences. It is not incontrovertible that transmission is not reduced by uptake, for the design reasons I put forward. -
Covid vaccine increases death rates!
+ SirBillybob replied to Alex.Blessings's topic in Men's Health
You didn’t say it, I said it; but it’s a clinical heuristic consistent with your initial stratification of health status and knowing such arbitrary status being an albeit flimsy basis of sorting out to vaxx or not to vaxx. Again, an arbitrary dichotomy of healthy vs unhealthy is not predictive of vaccination value. -
Covid vaccine increases death rates!
+ SirBillybob replied to Alex.Blessings's topic in Men's Health
This is specious. If you consider healthy status to be dichotomously yes/no (as you seem to suggest) a viral infection is by definition representative of compromised health. A common cold caught at baseline health, irrespective of that health, shifts well-being status to unhealthy on the overall gradient of health/wellbeing. Nobody can possibly know what huge array of personal complex variables predispose them to morbidity and mortality upon CoV infection. As such, it would be ludicrous to stratify one’s potential benefit of vaccination according to knowing something essentially unknowable. The suggestion to bypass vaccination remains absurd. Science without logic falls flat.- 100 replies
-
- 10
-

-

-
-
Covid vaccine increases death rates!
+ SirBillybob replied to Alex.Blessings's topic in Men's Health
Did you post research supporting this elsewhere? I am credentialed and have not come across any convincing data that underpins the assertion you just wrote. And exactly what proportion of deaths are followed by autopsy?! Obviously the risk is much less, to be sure. And while vaccination may be less imperative it offsets transmission to loved ones that possess higher morbidity/mortality risk. I just don’t see the point of this post and it is unrelated to the Florida data. -
Covid vaccine increases death rates!
+ SirBillybob replied to Alex.Blessings's topic in Men's Health
The 84% increase for males in that age group was not statistically significant. It was based on a total of 10 additional deaths than would be expected compared to the control period. That is 10 (rounded from 9.6) male cardiac deaths per hundreds of thousands of person years, among a huge age-specific population, above what would be exactly equal to the control period incidence. I don’t have time to estimate the excess rate (10 is the differential, not the rate) according to the denominators of Florida males vaxx’d from the get go. The lower bound of the confidence interval for 1.84 relative incidence is 1.05; take away one or two of those 10 deaths, legitimately due to common measurement error, and the lower bound drops below 1.0 … rendering the association meaningless and not clinically significant; again the inferential analysis lacks statistical power in the first place. Comparatively more overall population COVID deaths can likely be expected owing to the booster hesitancy this bulletin will spur. It would be easier and more sensible to spare single-figure cardiac death over some 18 months though lifestyle changes attenuating cardiovascular disease risk. What is particularly ludicrous is that the most convincing literal interpretation of the data is that neither gender age 25-39 should risk vaccination with ANY CoV vaccination platform on the basis of cardiac mortality risk. That subanalysis is statistically significant and the 2-fold short-term risk relative to the control period has a lower bound confidence interval much greater: 1.35 … much more measurement error required to nullify the association. However, it would be ridiculous to recommend no primary series or booster of any authorized platform typology for such a large proportion of the population. That science table is out to a buffet lunch. -
Just found him. No reveals; don’t ask. Latest IG Dec 2021; looks good. Latest FB he is a gogo hunk in a 2015 photo with other Gogo hunks. They often age out early 20s. I would say he is a genuine provider to make a more decent income than dancers. What your experience would be? No clue. He is quite short in stature but I think a dynamite body. I have not met him but he runs with a crowd of providers off the sauna brothel scene. You never know what you will get. I hook up with just as good looking guys in Brazil for $50-80USD in curated escort settings.
-
I used to follow the guy in these photos on Instagram. I cannot for the life of me remember his name since I had to streamline due to endless app ads that meant taking ages to scroll thru posts. So deleted many follows. Not that I would give his name but it might aid in determining his legitimacy.
-
Thanks, better. I don’t care about PM Hx.
-
My question has not been answered. I received 3 seemingly differently worded suggestions. I cannot think of a better way to ask it. Can’t somebody simply indicate what exactly I will need to do, if anything? Never heard of Firefox. I know what my email for the board account is. I use Google as my browser. I have never learned to change a password for any application. I have in the past retrieved forgotten passwords but due to the graciousness of related systems. Please use simple language and apply it to the Google platform. I have 12 years of university but nothing in IT. If mastering unfamiliar tech is the price of membership I will likely just drop out due to diminishing returns. Probably best if RadioRob manages this, keeping it to one person using one tech jargon format.
-
I just noticed today a request to confirm my email for this board, which I did. It was at the bottom of scrolling through topic headings. I have no idea what my password is because the board opens when prompted according to my handle and the password is never truly requested so my memory fails me. So, a bit confused. After the change, in which I think I enter my email rather than click on my handle when prompted, will I need the password or will the board similarly open by default without the password?
-
Would you only hire providers vaccinated for monkeypox?
+ SirBillybob replied to a topic in Men's Health
Chiming in … sounds more like a massage+ review than a MPXV-centric piece. Ontario? I doubt the provider is RMT. When there I had a few RMT providers give multiple sessions regularly due to a problematic back. Three providers over 25+ years; hundreds of appointments. The Ontario regulatory body, like any other certifying professional College (in Ont they are not called Boards, etc) would prohibit sexual interaction no less vehemently than for a physician, nurse, psychologist, what have you. This guy could be hung out to dry and even sued by a client, however complicit. Additionally, RMT is title-protected and it is as illegal to advertise or claim RMT status as it is to claim for example physician status without the “College” license. I highly doubt this escort is certified or aware he is treading on thin ice claiming such. I suppose he could say he is “professionally trained” in massage therapy. Or he may be “registered” in his own mind because he had a crash course at some point. I realize that I am splitting hairs if he dances around his true qualifications and how he articulates them, but there are strict laws about how this is represented. (Writing from Colombia so $500CAD seems outrageous LOL) -
I have been to Colombia recently. You must do their Check-Mig health declaration within 72 hours of your arrival, note arrival, not the boarding date and time. This application can be very temperamental, so be prepared to possibly sweat it out prior to successfully receiving the receipt with some of your data. Read about it online and consider viewing some YouTube tips. Do an image search to pull up some examples of what your receipt looks like. It appears within the application and is not emailed to you. The airline in Montreal required it to board. You declare that you are CoV-vaccinated but do not download it on Check-Mig, but be sure to have proof at the ready at Immigration in case asked. And get this, you must do it again to leave Colombia. Eeesh. Ostensibly to manage exposure of Colombians boarding flights out. And they are asking a few questions on the online form related to Smallpox (aka MPXV) as well; only about exposure / symptoms, NOT vaxx.
-
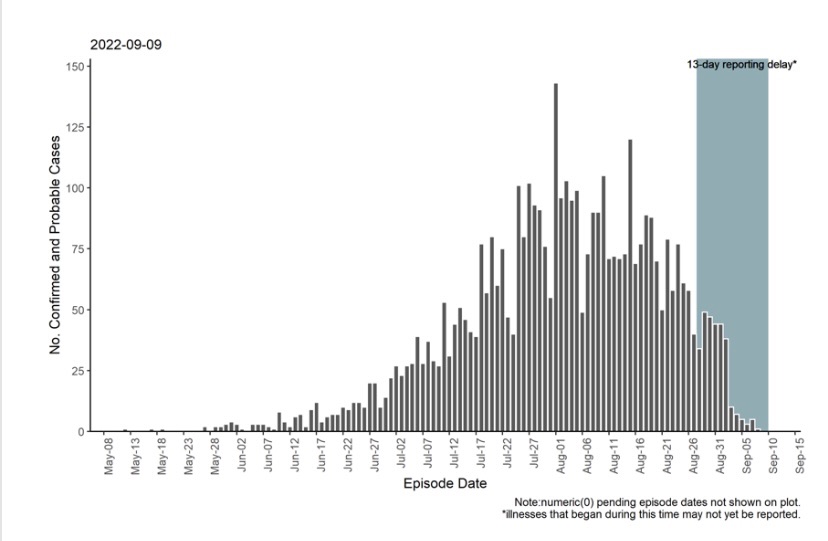
The paltry supply issued to Riverside County is disturbing, especially for those that want to be on the safe side in spite of substantial decline in case incidence in California, in which the Riverside case share is 5% (not depicted).

-
There are peers here wondering about a second booster, same situation as me. The Canadian guidelines do not recommend a second MVA-BN dose for most of us, that is, a boost dose single-figure weeks following prime for previously VARV unvaccinated or 2 consecutive boosters with a single-figure weeks interval for VARV-vaccinated decades ago. Moreover, the lack of access to a second dose is not attributable to vaccine supply chain; the guidance reflects best practices. That said, unrelated to stockpile or just-in-case imminent replenishing, I could neither get a second booster dose 8 weeks ago nor today if I wanted to. If you want to throw down, you could always challenge Canada’s immunization science table. But you would need to present detail that suggests you think just the right amount, not too much or too little. ————— For anybody here that accessed a 2nd MVA-BN dose, it is not ill-advised or contraindicated. My concerns about not accessing a second booster dose were minimal and further assuaged by Bavarian’s current publication of immunogenicity data that had already partially existed in the public domain. We now have a few sources of research that point to the residual protective benefit of the VARV vaccination that eliminated Smallpox.
-
The dosage is standard and the same for adults of all weights.
-
NYC monkeypox vaccine alerts -- 2nd dose -- 4 week window!
+ SirBillybob replied to Kevin Slater's topic in Men's Health
NACI concedes that common sense can override interval arbitrariness. It was expedient to administer Imvamune to circuit-break transmission. -
NYC monkeypox vaccine alerts -- 2nd dose -- 4 week window!
+ SirBillybob replied to Kevin Slater's topic in Men's Health
The Canadian guidance is bidirectional. As I wrote, unknowns about amplifying cardiac risk that is itself subject to demographic variables, as well as sorting out what product would be considered to have prompted, say, a serious adverse event if products are given too closely together. -
Bavarian Nordic has finally elaborately written up their old studies for Smallpox. A lot to unpack but corroborates my view of not needing to rush to get the 2nd MVA-BN dose. Let me put my situation this way: So my 1st Imvamune dose is a *booster dose post childhood Vaccinia & noninferior to 2 current doses for Vaccinia-naïve even up to 2 yrs, but a 2-year ^booster for the latter group then supersedes the former. The 2nd *booster for Vaccinia-experienced in childhood seems superfluous for now; can defer to an undefined date. The question, then, is when should we older guys pursue uptake of a 2nd *booster in order to more closely equivalize the titres conferred by a ^booster at 2.5 years (6 months past ^booster for the younger group), of course given unknowns about the correlation between immunity parameters and protection as well as crossover to Monkeypox immunity. https://www.medrxiv.org/content/10.1101/2022.09.07.22279689v1.full.pdf
-
NYC monkeypox vaccine alerts -- 2nd dose -- 4 week window!
+ SirBillybob replied to Kevin Slater's topic in Men's Health
Addendum: the above is deemed prudent but the imperative of MVA-BN ring PEP based on a defined presumed transmission event could logically override the delay. -
NYC monkeypox vaccine alerts -- 2nd dose -- 4 week window!
+ SirBillybob replied to Kevin Slater's topic in Men's Health
Yes, 4 weeks before and after, either sequence of the two products. As a compounding of risk is unknown and the confounding of attribution of an adverse event is greater the shorter the interval. -
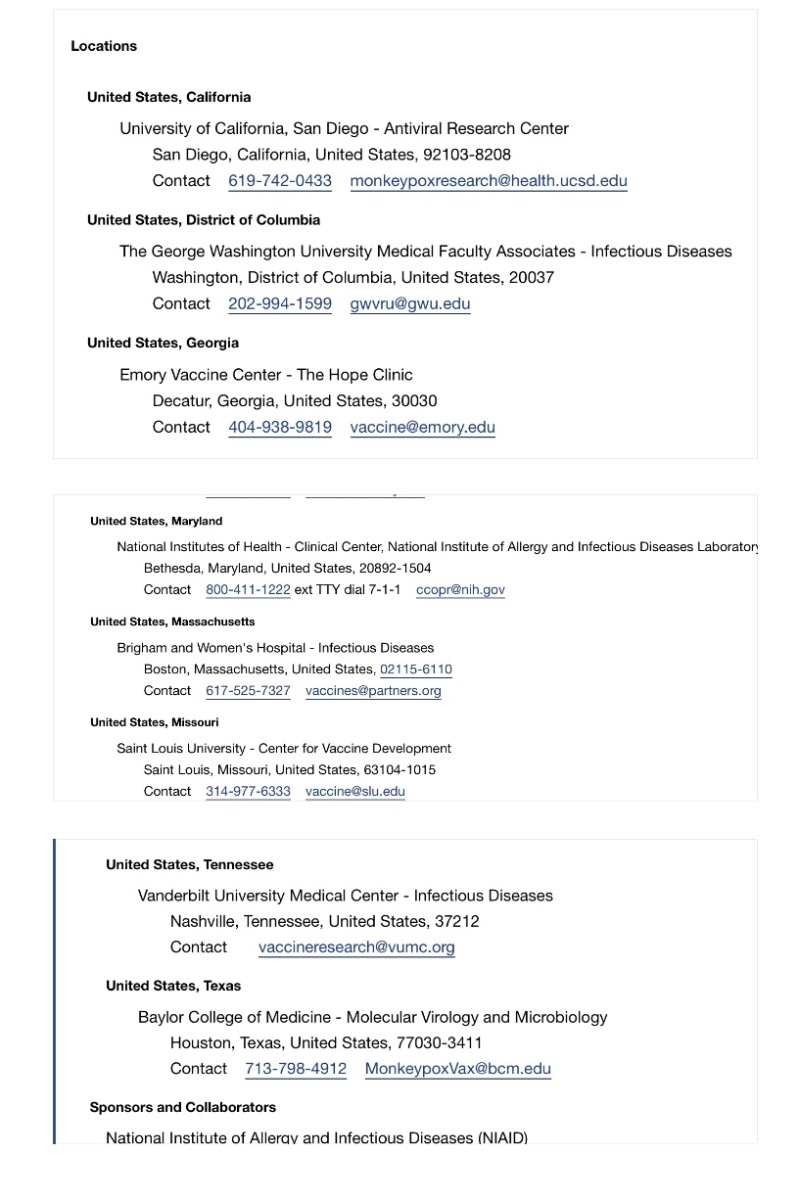
As promised, I am indicating the small Jynneos dosing trial is now open to enrolment: Subjects cannot have received any yet. https://www.clinicaltrials.gov/ct2/show/NCT05512949?recrs=ab&cond=Monkey+Pox&draw=2&rank=6
-
I follow it very closely. No, not yet. Possibly not at all. It will hinge on new case incidence trends, that seem to be dropping to about 1 case daily in 25,000 per capita wherein the denominator is adjusted to reflect the susceptible subpopulation. Additionally, the majority of MSM has not yet received an initial dose, likely mostly by choice and assessed risk factors. Another obviously relevant variable is current residual vaccine stock and anticipated future supply.