SirBillybob
-
Posts
3,823 -
Joined
-
Last visited
Content Type
Forums
Donations
News
Events
Gallery
Everything posted by SirBillybob
-

Question for those who've received the Monkeypox vaccine
+ SirBillybob replied to a topic in Men's Health
I wasn’t aware of this phenomenon. Could it be a ‘keloid scar’ that might occur for some not others? The CDC guidelines suggest the standard sub-cut dose over the new fractioned intradermal method for anyone with a history of keloid scarring. Reading between the lines, my tentative assumption is that a different location for intradermal is difficult to negotiate. I don’t know how easy it is to manoeuvre the preference of dose-specific format at point of care, or perhaps with a prescription. The risk then must be similarly considered for a 2nd intradermal. Might be simpler to fly in and out of Canada for the standard method, a decision also based on your interpretation of what might be better immunologically and as someone with childhood VARV vaccination. Whichever way, in particular for intradermal, make sure the vial has been swirled for homogeneity of doses extracted. Also your infection risk. I would probably roll up my sleeve now for the initial standard dose, if I hadn’t already a few months back, just because of the guidance, but I wonder if case incidence is naturally self-limiting and how much is attributable to vaccination campaigns. A dip in incidence is seen in Canada with about 20% of the target population having received at least one standard MVA-BN dose. A very substantial dip in case incidence in Spain is seen with merely 15,000 doses that reached only about 5% of the target population. -
Question for those who've received the Monkeypox vaccine
+ SirBillybob replied to a topic in Men's Health
It’s odd that so many have anterior forearm marks, since the fractional dose intradermal method in that location of the body replaced the conventional dose subcutaneous route quite recently, usually given in the tricep area where my swollen redness (and others’, posting the same reaction on line) occurred in that location but resolved quickly. But it may be that the P-town fellows had recent vaccination of the later method and less time to fade? I assumed the intradermal, one puncture, would leave a temporary wheal but not a lasting scar. I believe anterior forearm is the preferred location for the intradermal because those administering it likely tend to be experienced with Mantoux tests where I believe the needle comes in at the same shallow angle and with the needle bevel facing up. It seems to be a bit more technically demanding, therefore best invariant. Also, apply no pressure to the area afterwards that would problematically distribute the product subcutaneously. You know how for venipuncture we apply pressure even with a bandaid? That’s a no-no even if a bandaid is administered that might prompt a knee jerk reaction of applying pressure as for blood draws. -
I went to Campus this weekend for 75 minutes. I live nearby but visit very infrequently as I have not found it interesting for many years. I used to spend a lot of money there, hundreds per month, and my current disposable income is no less. This visit did not change my view. It was busy with all seating taken. It remains overall a good social space for gatherings of friends in a bar setting and the energy was good. I think it is fairly profitable for the owners. From arrival to a drink in hand took 55 minutes in spite of repeated signalling for attention. Not a problem for me as I drink water mainly, but a lot of patrons were getting up and trying to order at the bar because floor service was scant. This sort of deficit does not influence my venue ratings. Lack of service personnel is a known current chronic problem not necessarily related to management attitudes. The evidently impermeable plexiglass seal of the MSM private dance space seems misguided, if intended to obscure the area from gawking from the main bar. Air being the new poop, why compromise already negligible ventilation by creating a separate person-congested zone? An opaque hard partition perhaps with saloon doors, or fabric on a raised rod, either partly but not completely up to the ceiling, and leaving some open space above might have been more prudent to do the trick blocking views while better maintaining air circulation among the divisions. I wouldn’t personally vote to tear it out but it may have been a solution that could be deemed environmentally unsound. For all I know it may have been imposed by regulators of erotic entertainment disconnected from pandemic-related public health principles. Lest I be accused of venue favouritism, I should add that the other 3 stripper bars are not even on my radar.
-
Would you only hire providers vaccinated for monkeypox?
+ SirBillybob replied to a topic in Men's Health
You are very observant and correct to ask. Monkeypox reinfection potential is unknown. Smallpox immunity was not guaranteed but considered to be durable. Smallpox reinfection could not be easily observed in a world eventually without disease. But apples oranges. I should not infer either equal or superior natural immunity over vaccination immunity because little is known about either reinfection or breakthrough infection, or for that matter transmission potential coinciding with an undetected asymptomatic post-immunity infection. That said, I might prefer interaction with someone having recently recovered from seasonal flu compared to someone not infected (or yet infected should they eventually get and shed it) during an outbreak even if vaccinated. Flu vaccination is considered to be leaky and we know it and know it well whereas we don’t know much about MVA-BN and are far from knowing about it well. If you don’t want to catch Monkeypox, don’t engage in the behaviours that potentiate infection. A provider declaring recovery from Monkeypox must weigh the unjustified stigma clients reading the ad might project onto that information in addition to the ambiguity regarding risk. In contrast, completed vaccination status has a flavour of self-efficacy as if the protection conferred can be taken to the bank. Both sides must weigh risk in the context of WHO guidance that underscores that assumptions of recent natural immunity provided by infection in the current outbreak are unsupported. However, I had raised natural immunity because the trend in the thread is that providers might be sorted according to vaccination status, as if that track to protection had been established. Yet the category of natural immunity had not been mentioned and AFAIK recent recoverers are not deemed candidates for vaccination and cannot declare vaccination in the way that others may as a prematurely assumed advantage in ads. Neither inferiority nor superiority of one immunity track over the other is established. All this said, I tend to evaluate estimates of risk according to background case incidence. [As well as the ‘probability minimum one’ algorithm which I won’t get into here]. About 1,300 Canadians have been diagnosed. Assuming cases almost 100% GBMSM and a per capita denominator specific to that subpopulation estimate the chances of diagnosed Monkeypox infection based on cumulative count to date were 1/200. With no mitigation and no assumed natural immunity (.5% of us) or artificial immunity (20% of us best case scenario, notwithstanding suboptimal efficacy) compared to Spring onset, the average probability of two consecutive infections is about 1/40,000 assuming reinfection is a thing, and presumably less given current prevalence as well as prophylaxis uptake so far. -
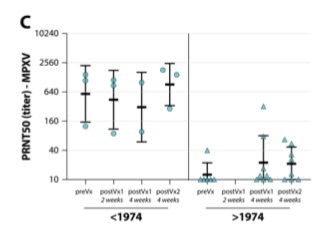
I think yours is the 1st critique. I didn’t think I was analyzing the article. Rather, I was responding to a request to try to summarize key points. But you can always go on Twitter where the article is being discussed somewhat and add your ‘two cents’, a colloquial expression not a commentary on your opinions’ value. 😉 I think “healthy” (in title) usually means no confounding by an underlying medical condition such as HIV. I thought they pointed out the lack of evidence of vaccination history based solely on age, and that it was an inference. But I think testing for Vaccinia titres was one way that inference was supported. But also look again at the slide and the pre-MVA-BN baseline titres for older age that seem to be explained by Smallpox vaccine cross-reactivity wrt to Monkeypox. I may be wrong, but I wasn’t aware of previous evidentiary support for an expected more robust response among Smallpox vaccinated relative to non-vaccinated. I thought there was evidence of an immunogenic response to Smallpox (not MPXV) from MVA-BN investigated in another article earlier in this thread looking at 1 versus 2 doses among older Smallpox vaccinated but that the antibody titres, as you yourself and others will say, had yet to be correlated with immunity to an exposure. And in Africa (DRC) MPXV outbreaks the attack rate was less. But no previous comparison of MPXV-specific humoral response to MVA-BN between the older presumably vaccinated and younger Vaccinia-naïve. Perhaps the recent unsurprising difference doesn’t nullify the value in exploring it. I didn’t think that the authors alluded to uptake rates for achieving control. If the not unreasonable idea that lower levels of uptake may adequately suppress incidence and spread, unlike say for CoV, then the fractional dose strategy for aiming for hypothetical coverage of 100% of MSM may be overkill in the interest of getting it to all of this sub-population but at the expense of immune response. But who can know the ideal sweet spot of dose frequency/quantity and uptake percentage? Again, about 20% targeted uptake in Canada at one dose for the ‘immunocompetent’ and two doses for immunocompromised category seems to have an effect on incidence, though an uptick of reported cases past few days.
-
There’s a potential indirect upside advertising advantage as he has, or will have, cleared infection, rendering further transmission remote to nil.
-
I tried to pick the slide out of many dizzying figures that will generate the most buzz. The Monkeypox neutralizing antibody titres (though very small therefore non-representative samples), as you can see, are much lower for the younger recipients of MVA-BN (aka Imvanex as it’s Europe). I do believe that the time series is not within-group, but based on a random selection of 33 samples across the vaxx trajectory. In other words, for the older folks on the left, for example, the 3 samples at baseline are not from the same 3 people as measured at 8 weeks. But it shows the trend.

-
Well it’s extremely detailed and geared to the Immunology/Virology academic crowd. It also focuses on Vaccinia Virus and Modified Vaccinia Ankara neutralization by MVA-BN vaccine in addition to the antibodies generated against Monkeypox Virus by the MVA-BN vaccine. The sample numbers are low. I take from it that immunity for all MVA-BN vaccine recipients falls short of the immunity conferred by actual Monkeypox infection. There may be some advantage to current vaccination for those that have a history of Smallpox vaccination but the degree of protective immunity lacks equivalency to acquiring and recovering from currently circulating Monkeypox. The apparent “strikingly” worrisome finding is poor MPXV antibody yield among MVA-BN recipients (ie, generally born later than early 1970s) with no history of Smallpox vaccination. There is lacking research data on comparative infection risk for younger vs older. The results do not say anything conclusively one way or another about withholding of 2nd dose for childhood vaccinees. The article further underscores the imperative of fractional dosing research. It may also support the agenda of randomized control trials for efficacy, a concept so far avoided, wherein cohorts will be divided between vaccination and placebo, given the suggestion of poor vaccine immunogenicity that itself overrides ethical objection to the type of gold standard approach usually employed including for COVID vaccine development. One such trial has been registered in Spain.
-
The manuscript abstract is a good summary and I don’t know how I would word it differently, but I will try to find time to read the paper more attentively and make sense of the figures. I am particularly interested, like @Luv2play, in the SPXV vaccination history advantage as I received it as a child and 12 weeks ago (already!) one full MVA-BN dose. I believe the research team has high and credible stature in the Infectious Diseases science realm.
-
This preprint on MVA-BN immunogenicity should generate some attention and controversy. You can probably find a blurb on the gist of it on Bloomberg or other current media. https://www.medrxiv.org/content/10.1101/2022.08.31.22279414v1.full.pdf
-
Au contraire, it is being modified to include non-pandemic-related functioning that had been proposed for digital-assisted entry to Canada prior to the pandemic, such as currently set up customs declaration at many Canadian airports, though the physical kiosk option will likely remain. So it looks like the app is here to stay though adjustments as required for its pandemic purposes can be expected. By the way, there exists the option to enter Canada without using the tool itself on one’s smartphone. The components just then need to be completed manually on arrival. It is not the law to use the app, but it is the law to satisfy the requirements that the app itself can record and generally facilitate faster and smoother arrival. Those that consider the amendments a bait-and-switch may be belly-aching about privacy concerns specific to the customs/immigration aspect that they did not get to more formally express in town-hall fashion but I expect they will be able to clear customs the old way.
-
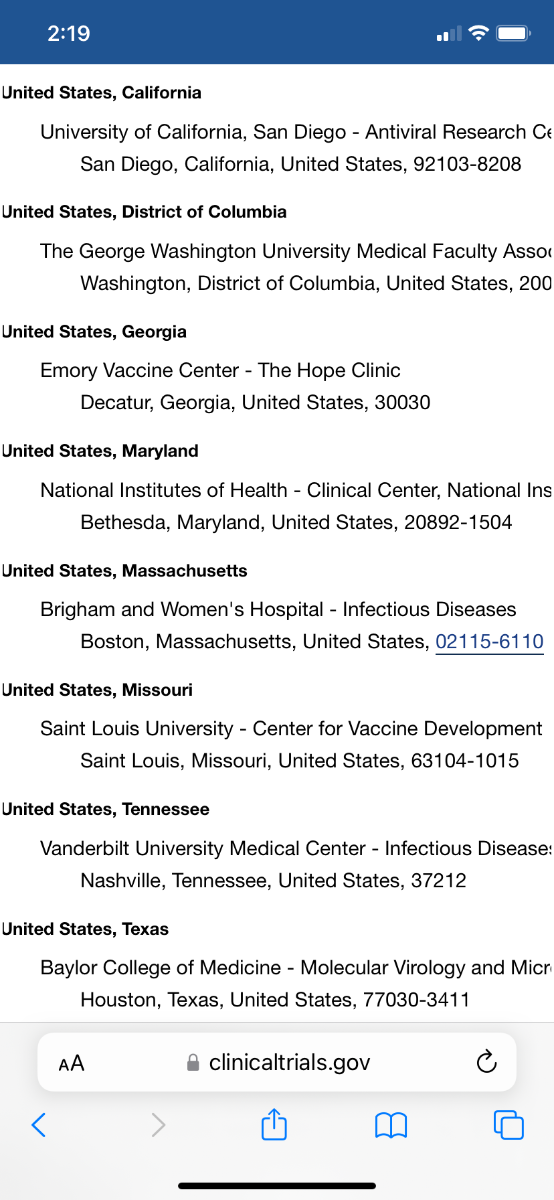
The small USA Jynneos dosing study should be up and running very soon. Summarized in link. It’s not recruiting yet but I’ll post the contact information for sites when added, IF that is the recruitment strategy aimed at the general public. It usually is, unless each location recruits within jurisdictions and in any case they should have no problem quickly filling up available spots due to location population density and motivation for two doses. I also attach a screen shot of the planned locations. A bit cut off on the right margin but you can open it in the link as well, Contacts/Locations. It is an immunogenicity study and may be also of interest to adults of any gender or sexual orientation that would likely not otherwise qualify for Jynneos in the near future but wish to contribute to the science agenda. https://www.clinicaltrials.gov/ct2/show/NCT05512949?recrs=ab&cond=Monkey+Pox&draw=2&rank=5#contacts
-
Early surveillance study suggesting asymptomatic Monkeypox infection is possible from acquisition through to clearance. Potential for viral shedding and transmission remains unknown. Proportion of asymptomatic cases relative to total cases remains unknown. A similar study, but adding throat swabs, is commencing at Montreal sexual health clinics. https://www.acpjournals.org/doi/10.7326/M22-2183
-
Yes, the worst case scenario among the Smallpox studies for MVA-BN 2-dose 28-day interval referenced in guidance is desired seroconversion % rate at high 60s (some studies in the 80s) at Day28 and sliding up to high 90s at Day42. For HIV poz the picture is far worse for the interim period, as low as 10% seroconverted by Day28 but then big bump up in % seroconverted by Day42. For that subgroup in particular there is a bigger climb to possible but more likely immunity following 2nd doses, suggesting the imperative of full regimen and importance of not shortchanging wait time to encounters subsequent to the 2nd dose. The Reddit OP did not indicate HIV status. That said, desired seroconversion rates, if you are restricted to a single dose for the time being, are better at 28 days compared to 14 days. The above points pertain to data for folks with no Smallpox vaccination history.
-
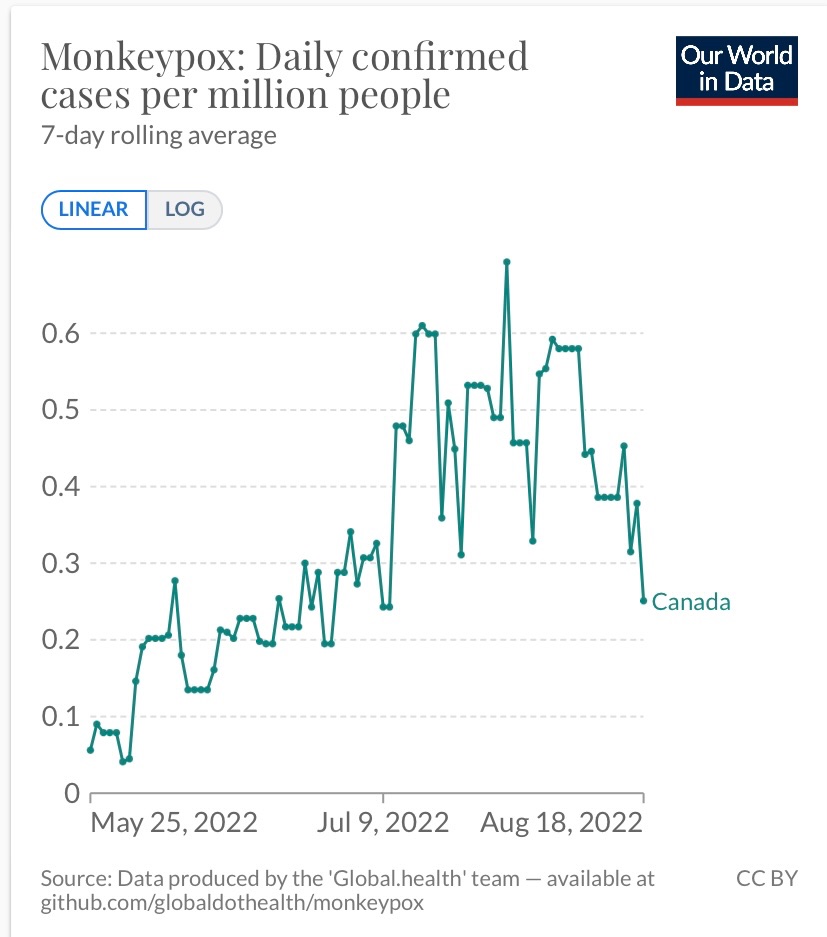
Signs are that Canada has turned a corner this month regarding MPXV incidence, with a single-dose MVA-BN vaccine strategy and uptake by no more than 20% of the targeted MSM population. I believe the UK picture is similar.
-
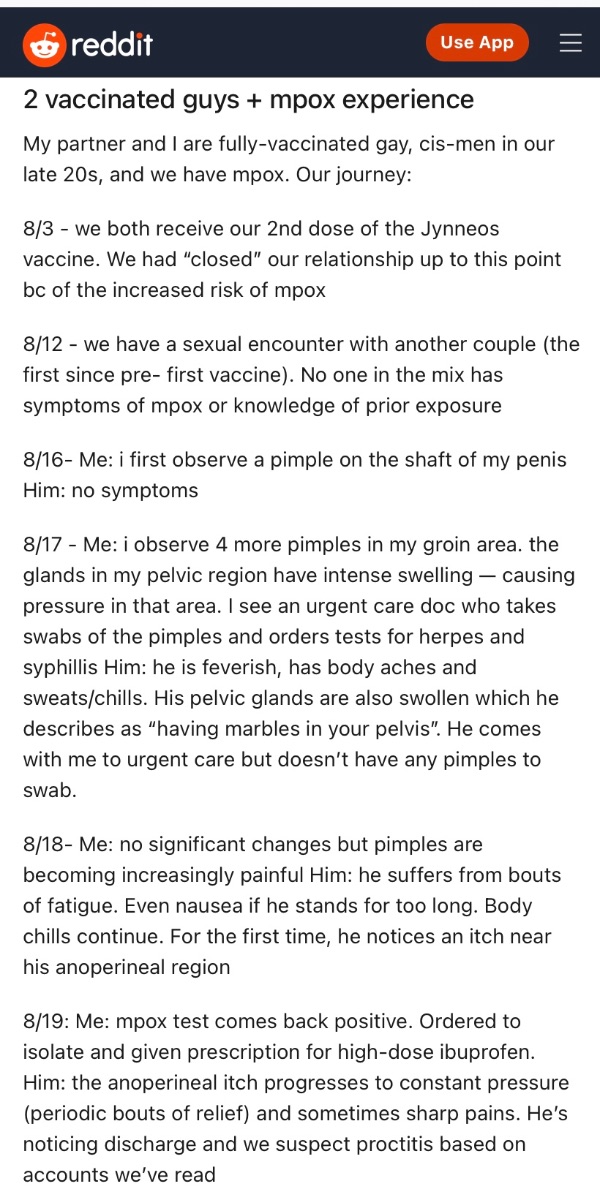
Right, this Reddit post is certainly lacking the reporting precision one would want. In follow-up commentary the OP answers questions about usage of conventional protection during the encounter ambiguously, and thinks the other couple had received a single Jynneos dose. If condoms were used along with minimally one vaccine dose for all four participants that should really raise eyebrows.
-
I received a spa mmessage but it had a happy ending. [I’ll let myself out]
-
Recent anecdotal report of post-vaxx breakthrough; partners that both got infected, likely from transmission from hook-up rather than one to the other, though viral transfer can ostensibly occur any which way in a group encounter. Symptoms consistent with MPXV/MSM profile. However, ménage-a-quatre occurred only 9 days from 2nd MVA-BN dose (presumed both full doses, neither dose spared/fractionated for either partner). Hook-up presumably not vetted for vaxx status, presumably non-protected intercourse. If the invitee couple had similarly been vaccinated, then all bets may be off for current containment strategies. An anecdotal report is not nearly meaningful data, but fully fleshed out could potentially shed light on what info remains elusive to date.
-
There is no severity scale that can easily be developed, aka symptom gradient, level, what have you. Mainly because there are two basic stages. First: prodomal (in the case of MPXV sick with symptoms other than dermatological and that could be common to other illnesses) that would require deciding on symptom count and level, perhaps duration as well. Second: dermatological (rash, lesions, &c) where a smaller total count for somebody can be worse and more threatening due to location on body, compared to somebody else with far greater quantity of dermatological involvement but in less vulnerable locations. If there is a randomness to where lesions occur on top of lesion quantity that factor alone defies a convincing comparison of symptom presentation between the vaccinated and not vaccinated. It appears that hospitalization alone, that might itself factor into a severity grade, is influenced by the location of lesions. Complicating this is the emerging trend of specific localized dermatological involvement among MSM. This adds the component of localized pain with an additional severity grade. Following that, the psychosocial implications of pock scars, and so on. Additionally, symptoms may respond to antiviral treatment but that attenuation may differ among individuals and according to timing of post-infection treatment introduction as well as access equity. Antiviral treatment may offset symptom severity that would have otherwise manifested. It was much easier to devise a severity scale for COVID, with consensus among scientists, for example to integrate into clinical trials.
-
Would you only hire providers vaccinated for monkeypox?
+ SirBillybob replied to a topic in Men's Health
Any provider could be among the 10,000+ confirmed infected so far, possibly multiples of that depending on undercount. It appears that minimally 1/150 of the hypothetical at-risk have or will imminently have natural immunity. Therefore, the question is whether they have bona fide immunity versus comparatively questionable artificial immunity, assuming the former reflects true disease clearance. And will a provider want to report having recovered from infection? Two levels of documentation a client may appreciate, one of them subcategorized according to dosing? It’s all very flaccidizing. -
On intraderrmal … https://t.co/L51qGy4F8V
-
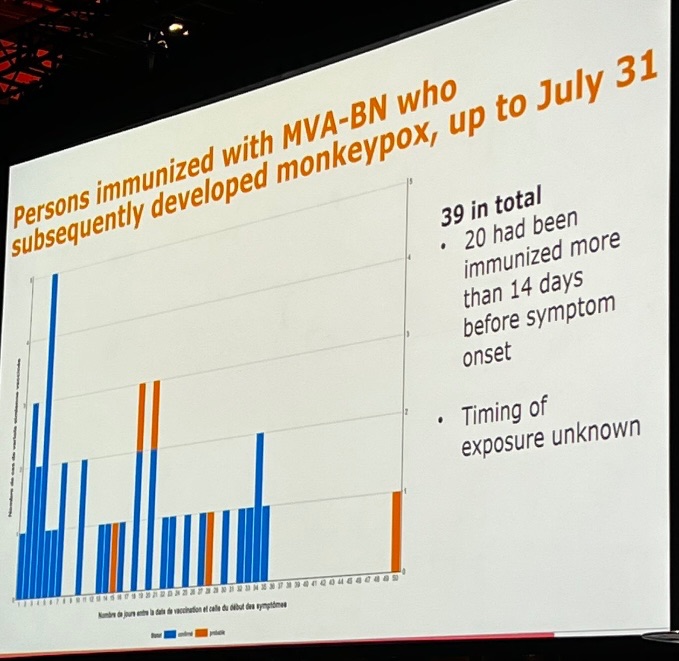
Montreal reports 39 breakthrough cases of MPXV within 15,300 mostly single-dose recent MVA-BN recipients. It does not tell us much as any or all cases may have simply been vaccinated too late following an exposure, and the proportion of those vaccinated that would have high behavioural exposure risk is not known. I cannot get a clearer slide for the histogram. Y-axis is number of persons (0-5) for each day following vaccination. X-axis is number of days up to symptom emergence following vaccination. Mostly confirmed cases (blue); a few probable (orange).
-
Preprint from France just dropped. MPXV PEP and breakthrough cases. Maddeningly, there were 2 SPXV-vaccinated cases (obviously historically, and they received the single MVA-BN dose in this study) but the researchers did not specify them within the individual list of the 12 cases in terms of timing of exposure/dose/infection. It appears that many of the breakthrough cases received PEP too late to offset infection following exposure. https://www.medrxiv.org/content/10.1101/2022.08.03.22278233v1.full.pdf
-
The graphs and charts are taken from the related literature. I have been mindful of summarizing within this thread the gist of such illustrations. Some readers here will be able to read them. Others won’t. They are added to show that I am not pulling ideas out of my ass. There are ideas presented here on the board that I believe to be inaccurate. This is often a ‘pages passed from hand to hand’ or U of Google & Facebook College phenomenon. Some readers have little tolerance for grey areas. There are some media articles in which known experts’ views are either inconsistent with the published research and with what other expert reports contain, or perhaps misrepresented by the journalists themselves. This may reflect both human error and lack of consensus. The latter reminds us that experts fall into the trap of having answers that they sometimes really don’t possess. We should appreciate lack of consensus because it behooves us to develop tolerance for ambiguity and uncertainty. We are often called upon to make nuanced judgements for our personal situations. We know how to get and how to avoid Monkeypox. Check. It’s a relatively wimpy virus transmission-wise for adults, all things considered. It may be a challenge for many to refrain from behaviour that upticks the probability of catching it, but by now there is sufficient information regarding what interaction situations should clue us in to being at the point of flirting with the virus. MVA-BN and dosing, dose dilution prospects, etc. Well, I won’t summarize or add more at the present time. I think what is reasonably known has been covered yet there is obviously more to uncover going forward. Smallpox inoculation history. In addition to small dated bodies of research supporting the notion that diagnosed cases occur more frequently (aka ‘attack rates’) among the unvaccinated (hence, younger population), we now have tracking data for some 500+ cases, as described in NEJM. The researchers did not wish to interpret attack rate differences and did not explain why. Perhaps because they would have to assume all other infection susceptibility factors were the same between the older historically vaccinated and younger unvaccinated subgroups. However, we know the general population shares of age from census demographics, and can estimate that the total number of males 18-50 is roughly twice that of males 50-70. Therefore, the 10% older male cases occurred in a population subset about half the size of the younger population subset that reflected 9 times the attack rate (prior to adjusting for population share denominators) compared to the older, presumably majority SPXV-vaccinated group. Therefore, if 10 older males out of 1,000 older males were infected while 90 younger males out of 2,000 younger males were infected, this would mean that equivalent attack rates would require 45 (not merely 10) older males within 1,000 older males to be infected. The 4-fold difference is consistent with the Congo basin findings of 35 and 15 years ago. Irrespective of proportions of total population at any time that had had Smallpox vaccination … obviously higher percentages the further back in time to the point of eradication … the attack rates are higher for the unvaccinated. Now we need to patiently wait for comparative attack rates to emerge in real time MVA-BN rollout, or unfortunately in global regions where MPXV incidence occurs across all age groups prior to MVA-BN equity. There seems to be no clear way to rate disease severity and cross-reference to vaxx history or current dosing questions. For example, one lesion may simply happen to emerge randomly in a very bad location while another person may have much more acute skin involvement and for a longer period but not threatening vision, breathing, etc. Hospitalization to manage unique challenges may not be a good marker of severity for this reason. Severity of Monkeypox in animal research is based on survival vs mortality. The research reported in NEJM did a lot of detailed quantifying but did not come up with a meaningful way to grade disease severity.
-
Uncoupled - POSSIBLE SPOILERS WITHIN
+ SirBillybob replied to EastCoastBtm's topic in TV and Streaming services
Coincidentally, as Sex in the City is mentioned, Stanley was reading A Little Life at his Friday night Table for 1 outing. I just started To Paradise.