SirBillybob
-
Posts
3,655 -
Joined
-
Last visited
Content Type
Forums
Donations
News
Events
Gallery
Everything posted by SirBillybob
-

Bogotá, Colombia (December 2022/January 2023)
+ SirBillybob replied to + José Soplanucas's topic in The Americas
I have consistently stayed in Chapinero because it is accessible to all sights but also happens to be walkable to my preferred playbook of trade, St Moritz baths/brothel and vast eating options on the route as well as upscale groceries and walkable love hotels for hook-ups. The facilities for play at St Moritz are dreadful. I discovered that the north west facing side of the Holiday Inn at Carrera 7 & Calle 69 is quiet because otherwise the traffic can be quite noisy for sleeping facing Carrera 7 and other accommodations may be noisy for the same reason. It also has the essential mini fridge and microwave. Airbnbs east of 7 (or west for more selection) in the Calle 60’s may also be a good option. I booked a fantastic penthouse a few years ago with a stunning east view of the hills but it’s now off the platform. I liked Holiday Inn for the familiarity of the area but would in future return to Airbnb options, though actually I’m over Bogotá due to having max’d out the platonic side of my love affair with the city. For trade, Brazil wins, no contest when levelling nonsexual aspects of destination appeal.
-
Is it really all hell breaking loose, though? There’s no Groundhog Day -grade commentary on auto forums and the themes there don’t intersect libido and cash. All that’s being opined is that at a certain point any discussion of objective price and subjective worth is superfluous and gratuitous when it would necessitate a shaking off of criticism and devaluation whether or not the object of criticism were to be exposed to same. Moreover, a savvy advertiser is cognizant of the reality that such critique arises from a dismissible irrelevant few. It’s client yield that influences price. The topic may be unstoppable but tired and boring enough to align the brakes. ~ Herb
-
Au contraire, a leading question masquerading as a statement. It implicitly offers safety in numbers regarding the judgement. The ad asks for a leap of faith because he is making one based on viewer screening. OP leap of faith is that others corroborate a view of ad audacity as filtered through one subjective perspective of appeal against price. A more neutral approach would be to simply inquire a 411. You’d have yielded the leading question through introducing a starting gate with answers to a question that was not actually posed.
-
Cleanly, then: “Oh. My. Goodness! Fiddle Dee Dee! Waaaaaah! Wowza! Ooooomph! Clean them pipes, Mister! Don’t stop! Aaaah! Clean them into next Tuesday!”
-
How long does it take PreP to work for Tops?
+ SirBillybob replied to Constantine's topic in Men's Health
I think he was asking whether there’s a relationship between sexual position and number of days of PrEP pre-loading to confer equivalent pharmacological protection among the categories within the sexual position variable. This is a complex question because anatomical sites vary according to infection susceptibility and the degrees of drug concentrations and time on drug required to shut down replicating virus within mucosal tissue. So technically, there’s a theoretical basis for assuming less risk based on insertive sexual position, given receptive anal is 10-fold riskier than insertive anal, that itself compensates for the sub-optimal drug concentrations associated with sexual activity prematurity undertaken within the arbitrary, ie, 7 day, preloading rule of thumb. But this is really getting into the weeds and the guidance wouldn’t be easily packaged or consumable with this level of stratification detail. The risk arising from deviating from the 7-day preloading guidance may be mitigated by an impromptu transition to the 2 of 2-1-1. In fact, some guidance entities are happy with getting into the weeds on logistical tailored bilateral transitioning options between the two conventional uptake models. That said, efficacy isn’t the exact term as efficacy is calculated statistically from research cohorts and comparing two or more samples not representative of any one unique sexual interaction. Condom use also occurs among PrEP research subjects and may make the key difference for breakthrough infections that would otherwise have occurred. Undocumented condom use is a behavioural factor that supports efficacy confidence intervals as much as does the imperative of acknowledging statistical power and conceding less than the absolute efficacy metric. The all-it-takes idea regarding that low virion quantity that escapes prophylaxis is relevant enough to structure the guidance equally across the sexual position categorical variable. Where PrEP is researched and position assessed there are relatively few tops that aren’t sides. If all or most were exclusive tops the research cohort would have to be increased to astronomical numbers in order to achieve adequate sample power for meaningful statistical analysis of efficacy. The greater the background incidence of the thing the intervention aims to prevent the greater the reliability of the effectiveness result. Paradoxically, though, the value of 100% is that it can never be. -
Rapunzelo, Rapunzelo, let down your earlobe hair.
-
How long does it take PreP to work for Tops?
+ SirBillybob replied to Constantine's topic in Men's Health
That and Quiet 2: Even if adherent a re-infection will likely elevate viral load to above the undetectable threshold if not above the virally suppressed threshold. You may be essentially having sex with one or more previous D=T partners and he won’t necessarily know his TasP and U=U are subverted with an up-blip in viral load, maybe even transient superinfection, in spite of having been taking meds properly. A condom in my wreckedom if you please. -
Trapped in a tower?
-
I’d be more than eager to embrace the following tradeoff: an increased number of escorts that screen out based on client looks for an equivalent increased quantity of escorts I would screen in based on looks.
-
Yeah thanks for the Saturday nite back bacon on bagel or burrito cravings, bae.
-
Firstly clean and oil your keyboard for optimal smooth typing.
-
Lauderdale Club Visit (Johnsons, LeBoy, Boardwalk)
+ SirBillybob replied to MrDakota's topic in Male Strip Clubs
OK, Tony, I’m in. It usually takes me 10 or more. -
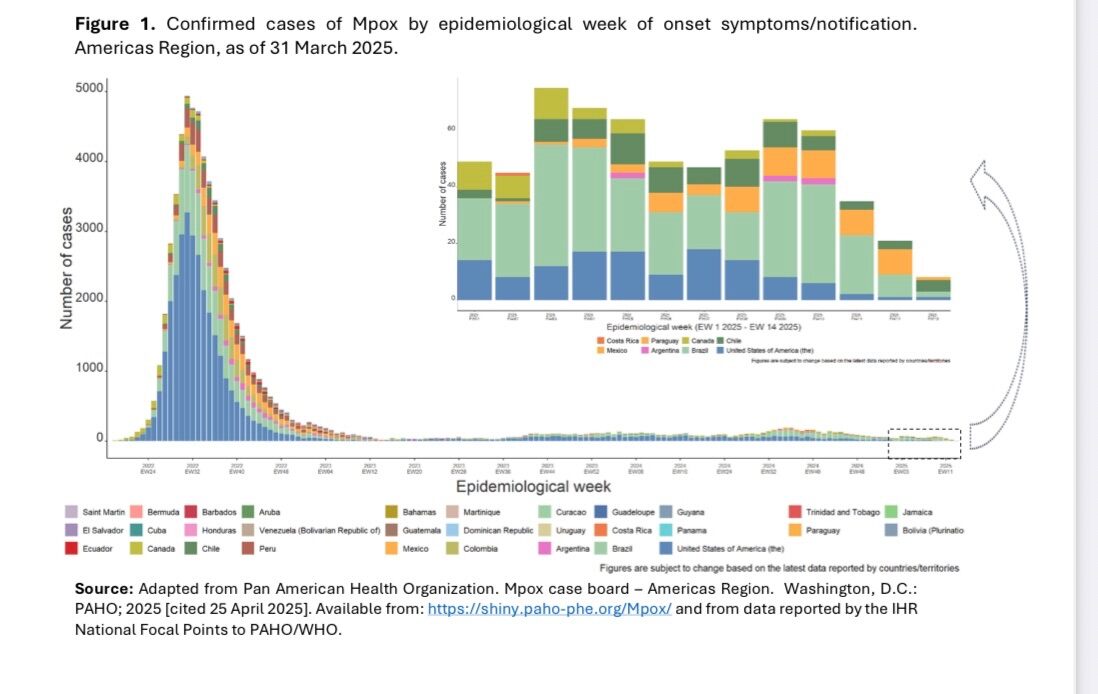
Here’s the link that enables views of Americas region trends less blurry than my screenshot. https://www.paho.org/sites/default/files/2025-05/sitrep-mpox-apr-2025.pdf
-
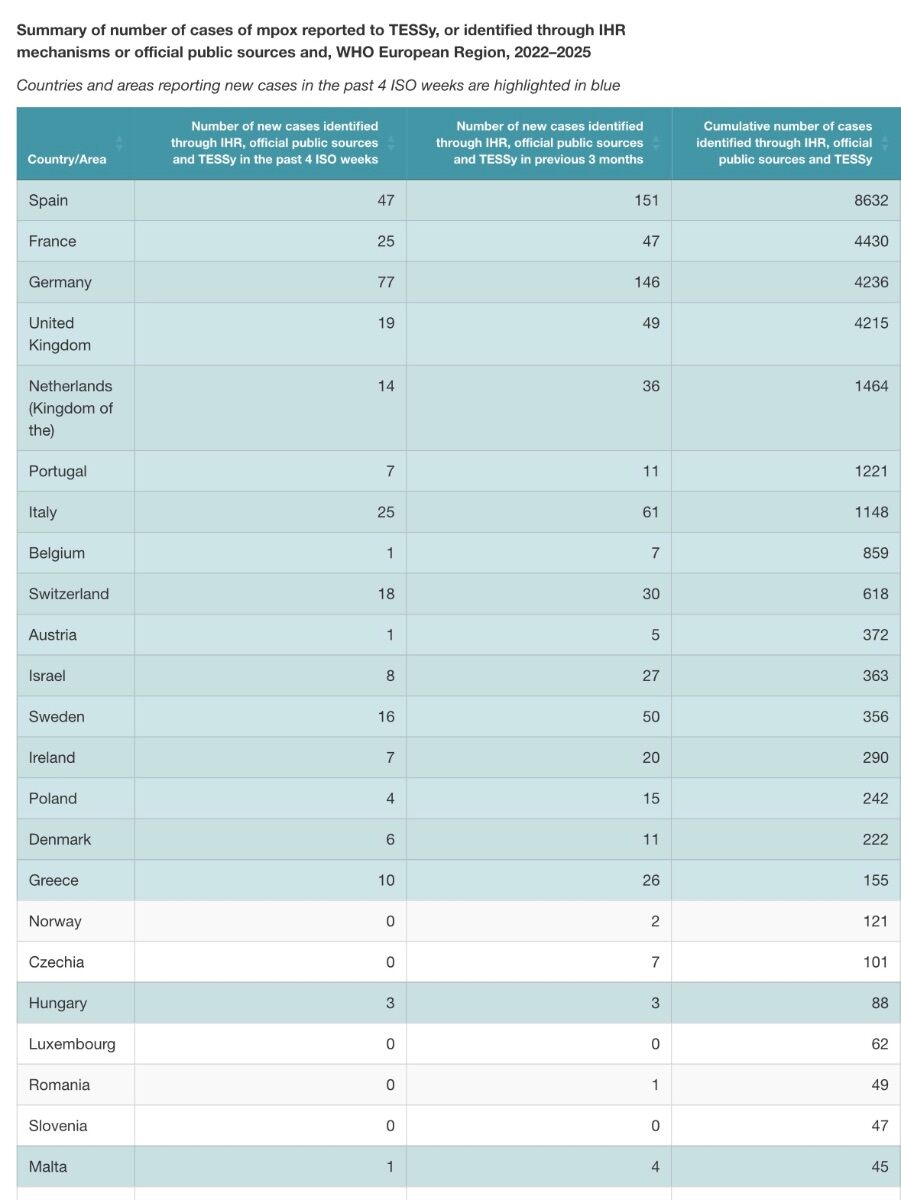
Use your judgement. Recent incidence trends are always available. Right now Spain, Germany, and Brazil appear highest risk and you can assess in the relativist context of peak rates, but nation-specific population denominators are absent in these metrics.
-
Time can fly on us. Are you sure 2 years ago and not when vaccine uptake peaked 3 years ago? In any case Canada’s national immunization guidance entity did not rule out booster doses of MVA-BN a year ago because of Mpox evolution trends at that time. However, just recently revised the guidance to state that a follow-up dose to the initial 2-dose series is not indicated at this time. In fact I took the 2nd dose last August because any time span between doses is permissible and I had been historically Smallpox vaccinated, as well as intending to escalate interaction 2024-25. However, you would be advised to pursue consultation about vaccine immediately if you have a suspected or known Mpox-infected contact, for post-exposure prophylaxis purposes, irrespective of your MVA-BN dosing in the context of the outbreak. As it’s often unclear it would be discretionary and depend on factors such as community incidence at the time. I doubt you would be denied if anxious following an occasion of intimacy. With trade I customarily inquire about vaccination because it makes sense when you are purchasing enjoyment accompanied by safety and offers an entry point for educating those at high risk yet poorly informed. What I do behaviourally, beyond PrEP to prevent HIV, and to mitigate STI potential crosses over to reduce Mpox transmission risk.
-
How long does it take PreP to work for Tops?
+ SirBillybob replied to Constantine's topic in Men's Health
Sure, whatever arrangement is within reach based on cost coverage and ensuring you have prophylaxis on board that fits your activity. My point refers to balancing the choice with when one actually needs infection protection, to the extent that one can predict those time frames. What are the diminishing returns? I would prefer to pay $1,500 annually for on-demand Truvada than receive injected Cabotegravir 6 times for free. But then with Cabotegravir I would also reduce or eliminate transmission risk during each 2-week tail phase within each 2-month block and also consider that it’s use may delay diagnosis of breakthrough HIV infection within a regularized testing regimen. No one option eliminates planning inconveniences. -
How long does it take PreP to work for Tops?
+ SirBillybob replied to Constantine's topic in Men's Health
You can decide together. But for me, infrequent sexual activity would be the determining factor that would predispose me to on-demand pills as it could be as simple as remembering 3 times across 3 consecutive days a few times yearly as opposed to 6 injections spaced apart in a rigid time frame, or optionally a few one-week dose loading iterations annually, scheduled by smartphone alarm reminder. 6 scheduled shots added to routine HIV and STI testing annually, being financial stable with no work obligations, would really cramp my travel planning. However, I am more than happy to forego risky sex in favour of satisfying intimacy, without feeling deprived and frustrated, but that does not call for prophylaxis if an offer presents itself that cannot be turned down. -
How long does it take PreP to work for Tops?
+ SirBillybob replied to Constantine's topic in Men's Health
Not how my doctor, correctly as per guidelines, prescribes Truvada (& it’s generic formulation) in all cases, as less frequent time-planned risk activity will dictate a tailored uptake, and transitioning from on-demand to daily, however temporary or sustained, will consider the drug concentration loading conferred by the initial double dose, reducing the absolute 7-day imperative. I’m sexually active, forever, and we settled on not taking PrEP daily, though I may at times follow the one-week dose loading as anticipatory substitute for 2-dose lead in for more immediate activity. In which case I have aligned with the daily PrEP option but never “forever”, just a few days following the final sexual activity that truncates daily PrEP. I and others fall within sexual activity scenarios that counter the notion of what daily PrEP in reductionist terms means. The uptake two-model binary is artificial. As my doctor puts it, one size does not fit all. My doctor takes the time to evaluate my risk factors, sexual activity patterns, adherence capability (given that on-demand poses unique requirements), and integrate renal health considerations, reminding me also that supplementation with condom use is the ideal overall prophylaxis. The topic question did not distinguish among uptake protocols or oral PrEP medications chosen. But yes, the recommended 7-day lead-in applies to either Truvada or Descovy where sex can be deferred for a week. Descovy is not applicable for on-demand PrEP. If you absolutely cannot defer risk activity, say, on Day 3 of lead-in dosing where you can postpone a spontaneous activity offer for minimally 2 hours and your doctor never clarified that you should transition to on-demand with an added dose at that juncture you were shortchanged valuable information. Unfortunately, die-hard thumbs-downers regarding the on-demand option have led some to conflate an impromptu transition to on-demand as running afoul of clinical recommendations. Have that extra pill accessible for drug concentration enhancement. In such a case my doctor adds that it makes sense to load the additional dose if it’s Descovy, notwithstanding that only Truvada is prescribed for the on-demand protocol. The reality is that some folks commence PrEP based on anticipated opportune sexual activity with pressing immediacy. -
Almost all participants in the Lenacapavir study acquired an STI at least once throughout their enrolment. Extremely high incidence buried in the supplementary data and not mentioned in the published NEJM central text. Your point is well taken because for oral PrEP routine HIV testing is usually packaged with CT, NG, and syphilis screening. Incidence rate about 80 per 100 person-years means that an STI would be expected to occur almost annually per individual particularly for unprotected receptive activity. Gonorrhea (40 per 100 person-yrs) alarmingly about twice per 5 years.
-
Not knocking PrEP. To be clear, though, efficacy in the research cohort of cis-gender MSM and gender diverse persons was 96%, with lower bound of confidence interval 82%, relative to background HIV incidence. No randomized control group as non-PrEP study arm assignment deemed unethical. The few infected had capsid resistance mutations; lenacapavir is a capsid inhibitor. Low but not zero chance of breakthrough infection. The 100% metric pertains to a study of cis-gender women.
-
Montréal trip report (and first post)
+ SirBillybob replied to londonfunlad's topic in Male Strip Clubs
I won’t have what he’s having. -
Succession meets Billions on steroids. “He can’t cut us; he can only shave us.”
-
Roaming travel dates are set manually by the escort. It is not some kind of AI formula. I had wondered and then asked Rentmen admin because the locations seem so randomly listed. That part is irrefutable. They are probably no more than market research by the escort investigating client interest, how much is in it for the escort, etc. Otherwise the patterns don’t make sense. My assumption is that this guy, on a 6-month visitor visa, will earn enough to justify staying in the popular location cities, so far New York and Miami his first 6 weeks to date. He has yet to hit the west coast. His extensive travel history of two dozen countries is not peppered with lower-draw tourist locations within his broader destinations. He is a tourist first, earner second to support the first. I think his locations will be driven by conventional tourism choices. I would bet on California and Hawaii eventually while the visa is active. If he’s smart, the Rockies, but perhaps to check a bucket list item, not necessarily to work.
-
Emmy immunity for Ellie it is, then.
-
Montréal trip report (and first post)
+ SirBillybob replied to londonfunlad's topic in Male Strip Clubs
Not that visibility ever mattered as private dances were years ago at tables in general seating and a lot could nevertheless creatively occur, prior to the current obsession of recording everything for visual posts, at Campus some time ago the plexiglass barrier was frosted with staggered opaque horizontal stripes. Cue the besides the point entry of the no camera rule. My point is simply a historical context for one’s assessment of privacy. I’m not the least bit exhibitionist but in those days it was a venial if not mortal sin to not offer one’s lap on which a hot guy could deposit self his perfect behind. One just suppressed overt expressions that typically accompany orgasm.