SirBillybob
-
Posts
3,822 -
Joined
-
Last visited
Content Type
Forums
Donations
News
Events
Gallery
Everything posted by SirBillybob
-
This is like, of all 4 eateries within a radius of a few steps of my home near the Quartier des Spectacles, only one offers the poutine I like while another serves decent frites. But the outrageous gall of a commercial infrastructure that fails to consider all of my requirements and preferences across all related venues. Although I suppose it’s good to know there’s an option to attend a venue according to performance guys that you categorize as female in one context, femme in another.

-
I haven’t had occasion to interact extensively with all people components of the acronym string that distinguishes a broad subgroup from the limited conceptual binaries of male / female and heterosexual / nonheterosexual, etc, and I haven’t experienced much challenge regarding my own categorization as a gay cisgender male, but for some reason I do feel a fellowship with the totality of subcategories within the aforementioned extended acronym. I don’t fully grasp why as I haven’t felt pushed into such an attitude or identity consolidation, and I harbour no antipathy towards the shrinking proportion of folks, fellow humans, excluded from the acronym. I think that it would confuse and subvert this identification and its mysterious value if I were to hierarchically stratify my sense of affiliation according to the various representations within whatever the acronym represents, or get caught up in the intersectional complexity of gender identity and sexual orientation. This doesn’t suggest that I’m always capable of resisting the unfortunate human tendency of ‘othering’ with respect to some aspects of mankind. That said, it does appear that heterosexuality alone does not dictate exclusion from the broadening spectrum of whatever best fits what any individual knows they truly are, but that reality doesn’t nullify the fact that not all heterosexuals are considered equally entitled to a claim to said orientation. Homosexual folks, in contrast, are not deprived of their orientation legitimacy, albeit at greater risk for proclaiming it, as it satisfies the criteria of problematic ‘othering’, the central core of whatever the “mean girls” colloquialism signifies.
-
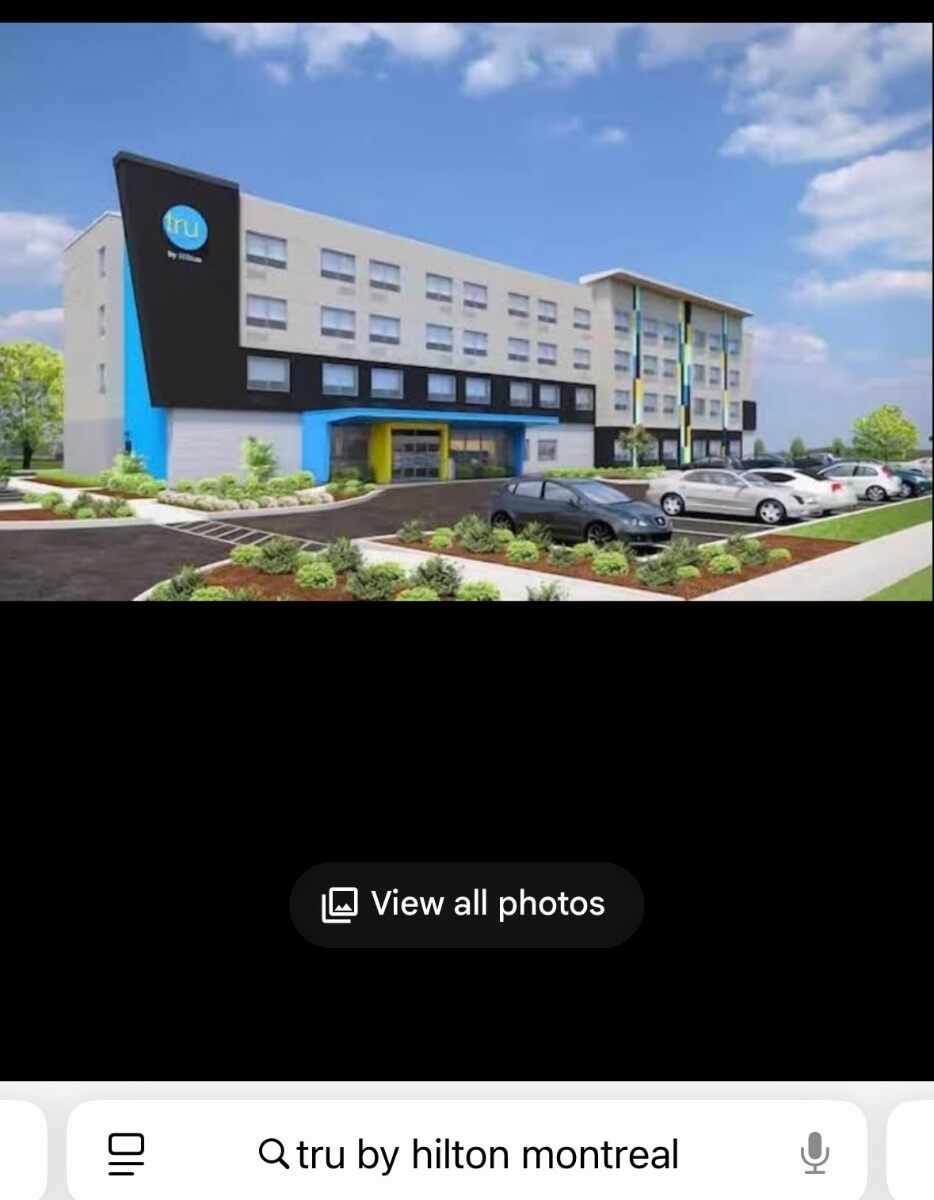
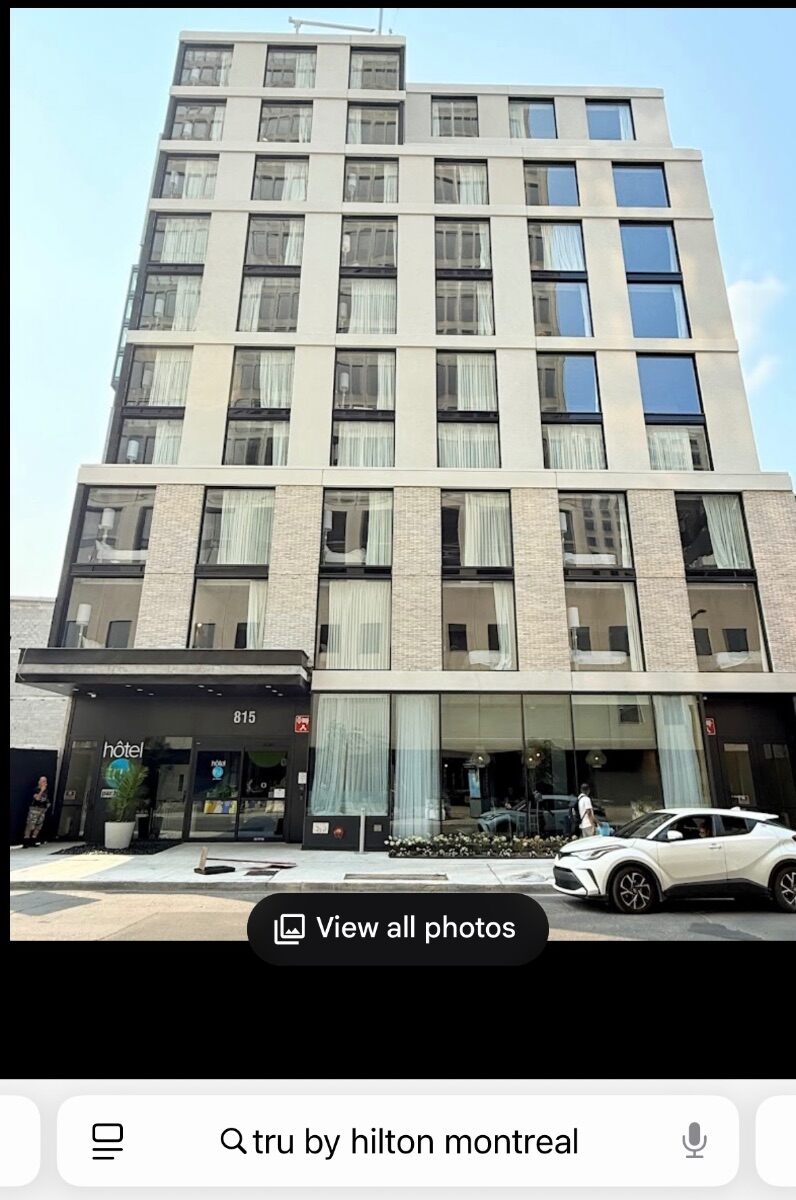
New. An older structure was torn down for it. Oddly, the design rendering associated with it is way off. Looks like San Antonio location. Whoever constructed the photo cluster must have entered it incorrectly … Untru by Hilton.
-

Former Stock/Campus dancer Tyson is advertising
+ SirBillybob replied to EZEtoGRU's topic in Male Strip Clubs
I know of him but never interacted. Agree his hiatus was extensive. He was working at Campus Thursday. -
Separate profile issue not the age verification one … today a day of firsts … subscribing to an OF dude, had been steered there thru a ‘scort platform. Both entities turned out fake with blend of faux stunning and obviously less attractive representations. I usually clue in better. Learned lesson, only $15. Time wasted with the guy: about 75 minutes communicating; that’s more aggravating. Back to Brazil it is.😆
-
Ahah … maybe cuz I wasn’t logged in and age verification could not be accessed thru my profile.
-
Not that I objected, but first time I had to enter my date of birth to enter an Onlyfans profile from a Linktree list. I think American.
-
Armpit appreciation thread, dedicated to Pitman
+ SirBillybob replied to marylander1940's topic in Legacy Gallery
My Movie 43.mov -
Sounds hot even if suggestive of the confounding product ‘Shrinkflation’ era. Not being a size queen, I’d trade off length and girth for uninflated rates.
- 1 reply
-
- 1
-

-
If you could go back in time with $1B and hire anyone...
+ SirBillybob replied to Merboy's topic in The Deli
To put it clangingly, turning over a new Leif. 🥰 -
If you could go back in time with $1B and hire anyone...
+ SirBillybob replied to Merboy's topic in The Deli
I think it’s almost a type of conceptual “clanging”, though not pathological. Like if the hotel artisanal toiletries included a rope soap that then could be considered employable on the king size headboard with one’s hire. I didn’t for one minute think that any posted comment was attributable to any fuddy-duddy who might be arbitrarily imagining the swinging 60s as their period of adult male peaking, but had assumed the Time Machine would not just be propelling my sorry old ass to the past while holding a device that might trigger a Cagney & Lacey SWAT team activation. 😏 -
If you could go back in time with $1B and hire anyone...
+ SirBillybob replied to Merboy's topic in The Deli
I’m gutted if he isn’t available now.
-
If you could go back in time with $1B and hire anyone...
+ SirBillybob replied to Merboy's topic in The Deli
Aaah, was it after all a lucre-pincher for which the term Achilles’ heel was coined? -
If you could go back in time with $1B and hire anyone...
+ SirBillybob replied to Merboy's topic in The Deli
So … examples of some of the most retired men as per the OP’s inquiry. -
But Oh, I just want a remote control for my curtains to match my carpet.
-
If you could go back in time with $1B and hire anyone...
+ SirBillybob replied to Merboy's topic in The Deli
Back to the billion dollar premise …
-
If you could go back in time with $1B and hire anyone...
+ SirBillybob replied to Merboy's topic in The Deli
Nobody made light of any historical tragedy, however close to home, by virtue of a random selected date. My graveside experiences in 1985 Toronto were not particularly silent and my erotic experiences not condomless. The proposition put forward is surreal and defies the characteristic of being realistic. Fantasizing Waikiki Beach 1941 between Thanksgiving and Christmas for a hot servicemen gangbang, in the context of the deliberately silly premise would, similarly, not represent being tone deaf. -
Or, “thank you” … YMMV
-
If you could go back in time with $1B and hire anyone...
+ SirBillybob replied to Merboy's topic in The Deli
1985? I would want … insist … that all the prospective encounters convincingly treat me as if I’m all shiny and new, like a virgin fucked for the very first time. -
Where there’s smoke there’s fire. If a subset of escorts on a chat site subtly or overtly self-describe as the best and most skilled and attractive options, consumers within the same arena will naturally tend to comment on such variables with respect to the broader constituency of escorts. It’s not necessarily shameless self-promotion because it’s just biz, but it does inherently lend itself to hyperbole at either end of the spectrum of subjective perception and critical appraisal of appeal, particularly within a monetary transactional context. Rarely do we read, “Ya know, that fella looks like he’d be an OK bet for exchanging cash to get my rocks off.”
-
If it’s actually ‘public’, not ‘pubic’, then I’m SlirBillybob or SirBillyblob, either of which could conceivably track.
-
I only freak out when I see the monthly statement for accommodating my fantasies. I have one of these …
-
Hunhh?
-
1. W’zapp 2. IDK 3. IDK … need a noon hour nap
-
With a carefully chosen deployment of emoticons you can make anybody like or not like you according to your whim, irrespective of positions on a topic. This only substantiates their artificiality and calls into question whether my own application of such reactions is honourable or disingenuous.