SirBillybob
-
Posts
3,822 -
Joined
-
Last visited
Content Type
Forums
Donations
News
Events
Gallery
Everything posted by SirBillybob
-

Providers asking for a client's professional services
+ SirBillybob replied to Ali Gator's topic in Questions About Hiring
A brochure indicating freebies for sweet helpful guys assisting with brochures? What about this suggests you’re not a pro? -
Is working as an escort very risky?
+ SirBillybob replied to charmasianman's topic in Questions About Hiring
IDK but the sure thing is it gets frisky. -
So how long was it since that last time since you’ll see him again? 😈
-
So, the answer to the OQ was an answer to the Q ‘what do u make of this ad’?
-
*Does ANYONE look like their pics ?
+ SirBillybob replied to Chancealot's topic in Questions About Hiring
… then on the woody. -
Providers asking for a client's professional services
+ SirBillybob replied to Ali Gator's topic in Questions About Hiring
Resuméing the thread here🙋🏼♂️ To whom do I submit my paycheque deposit deets.
-
You may already have a spidey sense of what 50 Euros will get you in terms of quality of trade. This is usually quite an accurate anticipation and those that repeat visit will have found their nirvana nevertheless, if not more the type predisposed to riding out lengthy patient periods of hanging out. YMMV.
-
I have none on Ignore coming up to 7 years as of next month. Here’s hoping a dude happened to be named Amos (I vetted thru member search to avoid offense) or a problematic aunt does’t trigger an itch. ScreenRecording_05-27-2025 23-21-14_1.mov
-
*any updates on the now infamous Austin Wolf?
+ SirBillybob replied to excelntsvc's topic in The Lounge
I think there are cases of crimes like this, viewed as egregious, when circumstances result in the convicted man to be released into the care of a responsible parent. That’s an outlier of course, but even rigidified-seeming guidelines are shiftable. -
*any updates on the now infamous Austin Wolf?
+ SirBillybob replied to excelntsvc's topic in The Lounge
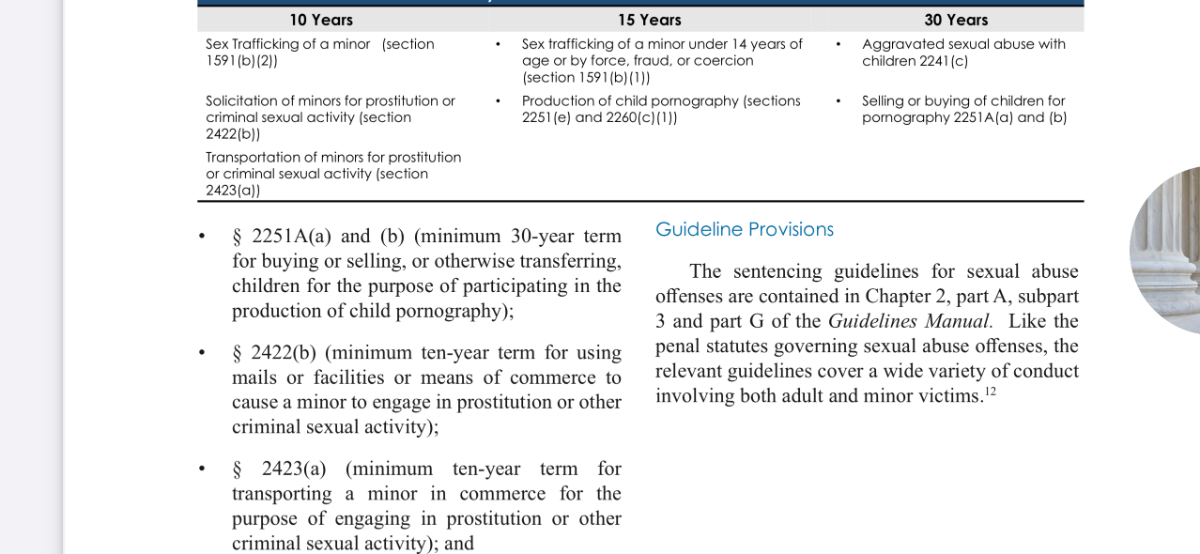
Base offense level 28 is up to 8 years sentence with lowest rank of criminal history, and criminal history hierarchy can escalate sentence length but I think his rank is I (lowest). Offense level points can be added to 28 according to Part G commencing page 204, but I don’t think he meets the criteria for many more offense points. That said, perhaps computer use in the crime as a factor adds about 2 years due to offense level rise to level 30, so it seems that is consistent (coincidentally?) with the mandatory min of 10 years. I think it’s the add-on points to 28 that are the unknown. I might bet on 7-10 years minus time served, then probation, the factor of sentence serve proportionality for parole/ probation eligibility you mentioned, and cash fine. My take with a big side of:
-
*any updates on the now infamous Austin Wolf?
+ SirBillybob replied to excelntsvc's topic in The Lounge
https://www.ussc.gov/sites/default/files/pdf/guidelines-manual/2021/GLMFull.pdf -
Providers asking for a client's professional services
+ SirBillybob replied to Ali Gator's topic in Questions About Hiring
… 28 Days Later 😏 -
Providers asking for a client's professional services
+ SirBillybob replied to Ali Gator's topic in Questions About Hiring
I need to make the terms my wallpaper.
-
*any updates on the now infamous Austin Wolf?
+ SirBillybob replied to excelntsvc's topic in The Lounge
For 2422(b) I thought it would be 10 to life, with upward variance from mandatory minimum 10 according to aggravating factors and downward variance from option of life according to mitigating factors, so I wouldn’t hazard a guess. It’s also actually unclear to me if in-person sexual interaction occurred between the age-15 minor and Smith and/or a third party. And I believe that is a state charge never imposed. That (if) it did transpire seems to me to be an aggravating factor (Smith losing points) for sentencing as proxy for unimposed sexual assault charges, and that (if) it didn’t it seems to me that it would not be a mitigating factor (gaining points) because it would be absurd to imply it’s commendable to not having fucked the minor whose intended enticed role established by Smith was to be fucked. I gather the guilty plea is a mitigating factor but I suspect it does not yield downward sentencing variance from 10 but could yield downward variance from life. To me, it seems there are layers of cart-horse variables and I don’t know the algorithmic sequencing of such factors.
-
*any updates on the now infamous Austin Wolf?
+ SirBillybob replied to excelntsvc's topic in The Lounge
So, a run-on sentence. My specialty. -
Pornstar escorts: turn on, or turn off?
+ SirBillybob replied to muscmtl's topic in Questions About Hiring
… clues … and hope he can mustard the capacity to lay good pipe in the conservatory. -
Providers asking for a client's professional services
+ SirBillybob replied to Ali Gator's topic in Questions About Hiring
I’ve done extensive pro bono for non-escorts and limited pro boner for escorts. -
Providers asking for a client's professional services
+ SirBillybob replied to Ali Gator's topic in Questions About Hiring
We professionals have all been there. [I’ll let myself out] -
Providers asking for a client's professional services
+ SirBillybob replied to Ali Gator's topic in Questions About Hiring
FYI you can edit original post for an extended period of time following submission, even if an emoticon reaction had been submitted. -
"The Gilded Age" on HBO
+ SirBillybob replied to + poolboy48220's topic in TV and Streaming services
Whereas at the seat of Sidmouth, “fit” is slang that refers to how hot Duke’s little social-climbing sibline-splintering Gladiolus is when sitting, standing, or hectoring splayed. Refer to #3.
-
Relax. The #815 address photo is not AI-generated. —— No, just the Thurs front bookend of Labour Day weekend. JOAT street dance festival that weekend but not Village-centric.
-
Straw man argument, though, if trans legitimacy in belonging to abridged … LGB … is predicated on sexual orientation when it’s reasonable to assume that both cis and trans folks are subsumed, represented within, LGB. In the same fashion, as it’s a complex topic, attempting to deconstruct these meanings doesn’t necessarily assign the meanypants label to any one person. It’s the gratuitous embellishment of a point with a symbolic prologue that’s part of the problem, as if one needs to raise an alert, or signify that the point itself is will have been strengthened by virtue of having dissed the other ahead if it. That’s the signification of insult, not that an opposing point of view represents an oversensitivity or a person or group prone to overinsultability.
-
For reading: author with status Evan Imber-Black on toxic secrecy.
-
How exhausting it must be to have to count heads and venue floor distribution by gender while ponying up CAD$36 to do so and cutting into party fun time, pouring over a smartphone spreadsheet app. It’s really taking one for the team. Polytechnique.
-
That annoyance or boredom by even a tribe’s single individual is optionally a response with respect to this thought-provoking post induces the heartbreaking realization that the type of coalition-building needed to support all diversity and to shield all disenfranchised from mean attacks still has some way to go.