SirBillybob
-
Posts
3,822 -
Joined
-
Last visited
Content Type
Forums
Donations
News
Events
Gallery
Everything posted by SirBillybob
-
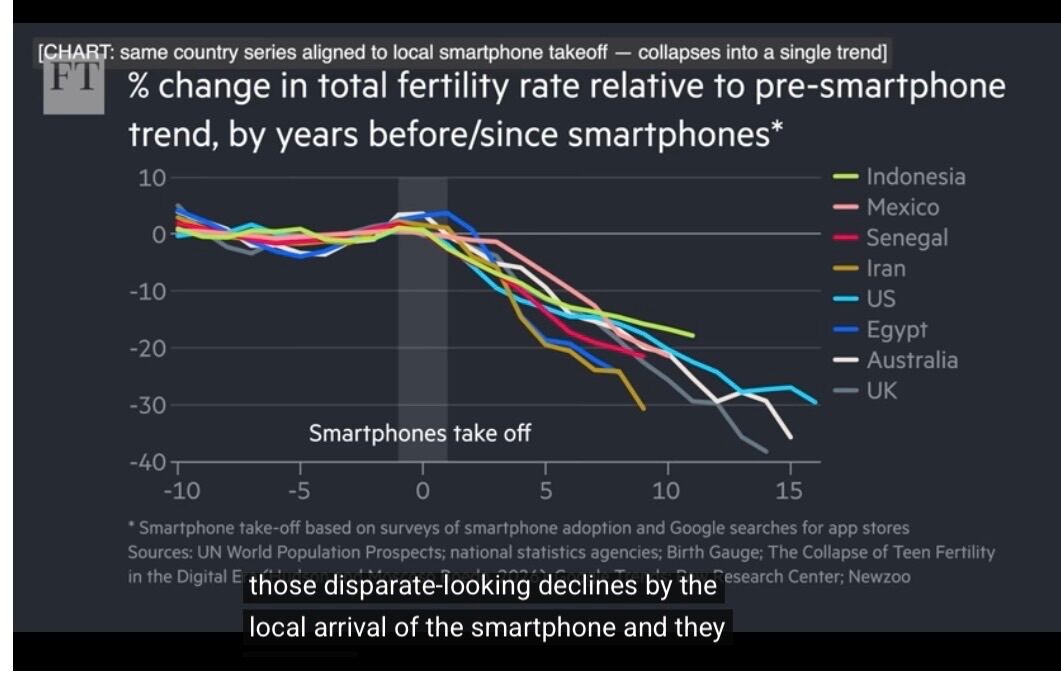
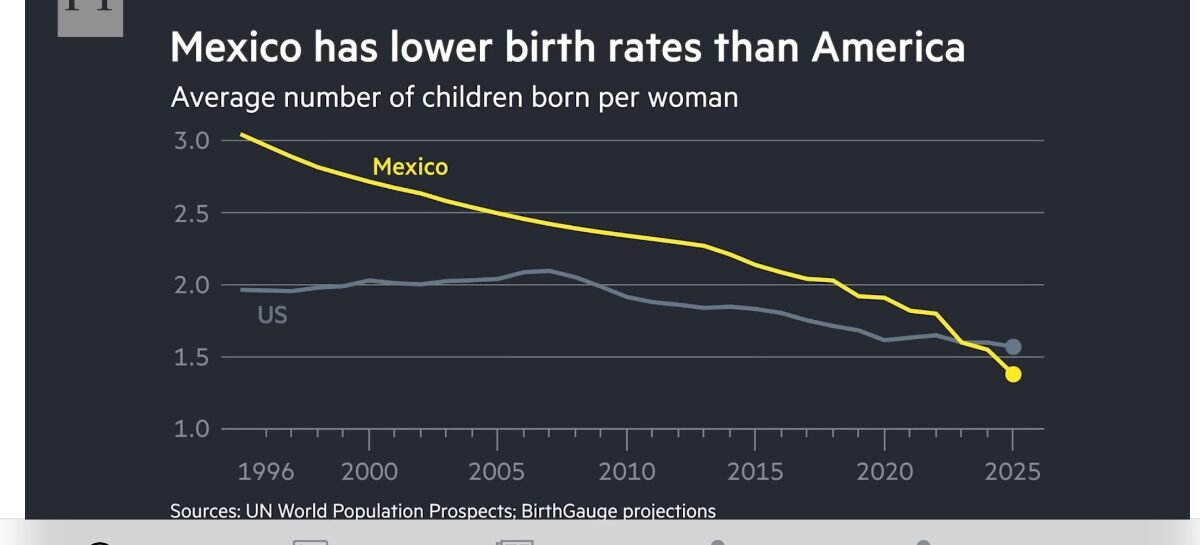
The key chart is misleading. It cannot be used as evidence that a smartphone inflection point accounts for an already pre-existing fertility decline trajectory that occurred for many of the countries depicted. By flattening one-decade pre-inflection fertility decline trends to about 0%, when some of those actually approach the same level of decline as depicted post-smartphone, as opposed to running temporal longitudinal trend lines through the steadily dropping fertility metrics that unequivocally cannot be attributed to smartphone prevalence, that history is falsely nullified. (See Mexico for illustration) That is likely an artefact of the attempt to adjust for national variation year by year in a single standard for estimating inflection influence. However, that distorts the graph, visually artificially elevating the true potential impact of smartphone availability, as well its scope of abruptness. At most, such device access can be considered as potentially accelerating fertility changes that had been, and continue to be, attributable to a host of other variables unrelated to the “tech shock” inherent in hand-held computers. The verbal presentation compensated by suggesting that the smartphone analysis can only speak to whether fertility fell faster than what might have been otherwise expected. Fertility transition had been substantially well on its way. For example, Mexico’s fertility decline rate is almost symmetrical around (pre / post) the proposed inflection explanation point posed by widespread smartphone uptake.

-

Cute Critters to Take Our Minds Off Everyday Stresses
+ SirBillybob replied to + quoththeraven's topic in The Lounge
13-second video. I had to double speed to reduce its size to attach here. Looks like the understudy for Tybalt, Prince of Cats, hadn’t read the brief for its entrance cue, or just wanted its moment. My Movie 24.mov -
Of course, rightly so. What do PrEP product monographs contain regarding condom use?
-
Sounds like an appeal for special insight that you apparently uniquely possess relative to certain others. That’s doing a lot of work rhetorically. Elevating the preference for condom use for insertive anal, particularly in a transactional context where services and health risk terms are commonly negotiated, to evidence that the client doesn’t understand close physical connection feels like it’s changing the subject from typical boundaries to that of flimsy assumptions about deficits related to grasping desire and arousal. Some bottoms find condomless sex more satisfying. Some tops find condoms preferable. (Here I use these terms insertive / receptive behaviourally rather than as defined person categories.) This isn’t to say that both parties’ access to satisfaction reasonably on their terms isn’t important. However, one wouldn’t expect the incompatibility to yield psychological trench warfare at point of intercourse. The reason the OP started the thread was that the experience was startling, truncating the type of encounter that usually plays out without drama. Nobody here that may view the ritual of condom application, its brief pause and associated anticipation, as intentional and relational has necessarily lost the plot regarding sex dynamics.
-
You’re serving common sense across a few behavioural health risks with inarguable cascade effects. This is familiar territory inn’t. Historically, sex has attracted moral scrutiny. But it doesn’t follow that concern about STI transmission is therefore a disguised sermon where the character of people making certain choices is condemned, or that inconsistency in other areas of wellness is hypocrisy. A parent whose health status is undermined by obesity or the dude whose flecks of puke land on your shoes outside the pub is nevertheless qualified to dissuade their family member from smoking. That STI health guidance is so frequently conflated with moralism may say less about the guidance than about the unique cultural space sex continues to occupy. Locked in a binary of virtue or vice, the discussion can only go in circles. And now I’m headed to the fitness centre where gripping barbells may have a desirable depilation effect with respect to the hairs on my palms, after which I may check out possessing an adequate supply of condoms.
-
Whataboutism and false equivalence much? By that logic, anybody regularly taking one basically established health-related risk such as a side of chips versus rocket at lunch forfeits the right to discuss another, along with weighing in on prevention guidelines and preferences, and gonorrhea checks your BMI before infecting you. Of course there is a value judgement regarding condom use, and public health messaging is inherently normative. Avoiding infection is preferable to acquiring one. In fact, it’s a rather uncontroversial values position. Recognizing it isn’t the same thing as demonstrating hidden moralism. You yourself may be inclined, with good intentions (how else would your motives be?), to discourage a guy’s smoking habit. Reality is under no obligation to be less carcinogenic in deference to his personal autonomy.
-
Are TELEGRAM GROUPS useful for discussing escorts?
+ SirBillybob replied to Roger Smith's topic in Questions About Hiring
I suspect it’s as much work to get laid thru it as it was to get cables laid for it. Lotta deep diving. -
Surprised and sympathetic. I’d have thought that decent trade was merely a local phone call away from The Luxor.
-
1st Male Supermodel Lost $4.5M to Doomsday Alien Sex Cult
+ SirBillybob replied to samhexum's topic in The Lounge
A housecat at the time probably filed a missing pyjamas report. -
That’s a lot of sudden turbulence for a penis wedged between the maxillary and mandibular arch. Spring-loaded cigar cutter equivalency, anyone? I thought not. Paired fellatio off the spindly legged table before the square-cube-law begins filing objections.
-
Low-intensity shockwave therapy applied to ED has been progressively on the menu for some 15 years. The jury remains out. There are a half dozen or more systematic meta-analysis reports that overlap in terms of the mainly same dozen or so clinical studies that are incorporated into evaluation as a collective. At this point I think it’s, well, try it if you have the resources. You can always self-administer the before / after questionnaires on function that can be found in the public domain, on top of subjective impressions of change. With no current registered recruiting studies to be found, perhaps a kind of equilibrium has occurred, outcomes just promising enough for the clinical option to persist, equivocal enough to forestall urological abandonment. At worst, you take your best shock and it ends up consigned to boutique medicine limbo. Of course also be wary of testimonials put forward by product entities. I also cannot comment on how the clinical literature translates to DIY home-use gadgets. Although clinical settings are using equipment, if consistent with published research, at a retail cost of $30,000+ 🤷🏼♂️ To access peer-reviewed journal articles: Google “shockwave therapy ED metaanalysis”
-
A Baby will be above my Apartment, am I screwed?
+ SirBillybob replied to Rod Hagen's topic in The Lounge
My air purifier is extremely quiet at max video recording volume. I can hear the street garbage collection and sirens (I live a few blocks from a main street artery). Such sounds drive me crazy without masking. First clip is all other ambient noise free, depicting what to anticipate from this model of air purifier (from Best Buy). Second clip is all other ambient noise free except the sound of ‘Big Water for Sleep’ iTunes track through a speaker a few feet away, though it’s more pleasant than recorded here. I cannot hear sirens or huge metal garbage bin slamming sounds from the forklift operations. And of course one can adjust the volume. IMG_8330.mov IMG_8331.mov -
If the outcall rate is steep, don't bother!
+ SirBillybob replied to viewing ownly's topic in Questions About Hiring
- the bespoke Kimberly-Clark deep tissue that prompts you to philosophically price the meaning out of money -
When bent over perpetually indulgently, always watch for flying objects that mistake you for the Guajataca Tunnel.
-
Any experience with these guys in Albany? Reyrl
+ SirBillybob replied to shoeshinej's topic in Spas & Masseurs
Virtually none.
-
A Baby will be above my Apartment, am I screwed?
+ SirBillybob replied to Rod Hagen's topic in The Lounge
… while also keeping one eye on the pond riding your cart to the pickleball courts, replenishing electrolytes after the game. In any case, diaper pails bring the thread full circle. -
A Baby will be above my Apartment, am I screwed?
+ SirBillybob replied to Rod Hagen's topic in The Lounge
Duh, how else would we have “See you later - “ … “In a while - “ ? -
Sorry. Miss.
-
A Baby will be above my Apartment, am I screwed?
+ SirBillybob replied to Rod Hagen's topic in The Lounge
Frankly, I wouldn’t catastrophize about the imminent screeching as I doubt it will be very discernible, if at all. Similar in decibel range to canine yapping but higher frequencies less likely to bleed through a floor/ceiling barrier. In contrast, a caregiver with an annoying thumping heel-strike gait (my pet peeve) may end up pacing around for long periods at all hours while carrying and attempting to soothe the tiny owner of said amazingly developed vocal cords. Months in, one of these wheelies (below) could be annoying if used on hardwood or tiles. Some folks find ‘white noise’ overrides as disturbing as regular acoustic intrusions but I live by them, for example a waterfall soundtrack loop from iPhone to a miniature-ish Bose Bluetooth speaker, both devices internally adapted for recharging abroad. Prior to that I used a machine similar to the one you depicted, a company called Marsona. Very effective. I see they are quite expensive; you might try the cheaper Marpac that has a twist swivel volume emission feature to see if you can tolerate it. They are standard for small waiting rooms to mask clinician-patient discussion.
-
Jorge in San Diego $88/hr (From Airbnb Services)
+ SirBillybob replied to + 7829V's topic in Spas & Masseurs
I’ve always appreciated hardwood in my Airbnb dropdown menu features. -
Thanks, I had accessed the full article. The page had the usual ad features and the Temu one was amusing. Most of the other ad popups were associated with gambling, similar in ironic potential. These prices escalations amount to forced errors, as if a penalty kick against you occurred while you were off knocking boots elsewhere instead of defending the net.
-
Opened the Post article and a Temu price-drop ad popped up. Internet’s irony either remains undefeated or the algorithm is pushing to restore sanity.
-
Thank goodness for content regulations that all but obliterate chatroom trench warfare.
-
Ebola can remain in the reproductive system
+ SirBillybob replied to Luv2play's topic in Men's Health
One question that emerges here is what implications for us, particularly given the blame game history affecting MSM constituencies. If a MSM transmission event were to occur and be understandably publicized when in fact the more likely outbreak seeding scenario would be MSW … the prospects being greater for a male survivor migrating beyond the outbreak epicentre being heterosexual … history tells us what finger-pointing to anticipate. The persistence science itself is well established, with much meaningful input from Canada’s epidemiological think tank in Manitoba, and has real outbreak-management implications. But in comparatively well-resourced regions, the more immediate concern would almost certainly be acute symptomatic cases and conspicuous transmission clusters long before survivor-semen persistence became the dominant public discussion. Those clusters would rapidly manifest within gen pop given Ebola’s R metric, say 2.0 minimally, in which sexual transmission is but one baked in route to infection. Ebola’s severity works against long silent propagation. By the time residual infectiousness concerns entered mainstream local consciousness, there would likely already have been multiple severe illnesses, hospitalizations, and recognizable transmission events much closer to home than abstract outbreak reporting from afar. That proximity itself would probably be the first thing capable of significantly materially upticking behavioural modification, including condom uptake among MSM individuals otherwise psychologically distant from risk. Of course one can mostly remove oneself from any outbreak rekindling equation by using condoms now. It’s not as if condom use trends to invalid. -