SirBillybob
-
Posts
3,822 -
Joined
-
Last visited
Content Type
Forums
Donations
News
Events
Gallery
Everything posted by SirBillybob
-

Birthday Etiquette With Your Favorite Provider(s)? 🎂
+ SirBillybob replied to + 7829V's topic in Questions About Hiring
I offer my calculator for the birth year component because unique leap year patterns arise from rotational speeds rarely dividing evenly into orbital periods. -
ObangmeCare? There’d be a need to redefine second opinions. I’d volunteer as tribute to beta test revisions.
-
You have identified the need to consider three separate issues, as well as possibly implications for how much reassurance to derive from: overall spontaneous clinical resolution prospects; specific AMR strain clearance potential compared to non-AMR; and judicious (even restrained) use of antibiotics, despite resistance risk, across a range of symptom severity and persistence. We know clearly neither whether AMR cases are equally self-limited nor whether or how much the subset of overall shigella cases that is severe enough to seek/need antibiotics overlaps with the subset least likely to respond to standard antibiotics. The pinch point clinically is the subset that is severe enough to warrant antibiotics or hospitalization (or both), but precisely where drug resistance matters most. Acquiring day passes for orgies is unlikely. Thus, the wording that asserts high frequency of overall self-limited disease and the notion that the trend of increasing proportions of drug resistance is consequential are not contradictory. They describe different slices of case distribution. Our mission, should we choose to accept, is to reduce fecal drift. Your point about transient infection is well taken, though, as annual case numbers reflect mostly spontaneous resolution and brief windows of transmissibility.
-
Along with same scheduling dynamics …

-
In which case it’s at the intersection of his labour and your party … whip optional.
-
Montréal trip report (and first post)
+ SirBillybob replied to londonfunlad's topic in Male Strip Clubs
Here in La Belle Province it’s renamed National Patriots’ Day (translated) since about 2003; beginning in the 1920s by yet another francophone name but corresponding by date to Canada’s Victoria Day, for long weekend uniformity. The point being counter-colonial. Elsewhere one doesn’t tend to see lace doilies perched on heads, but to confuse matters more O Canada was sung in Buffalo. -
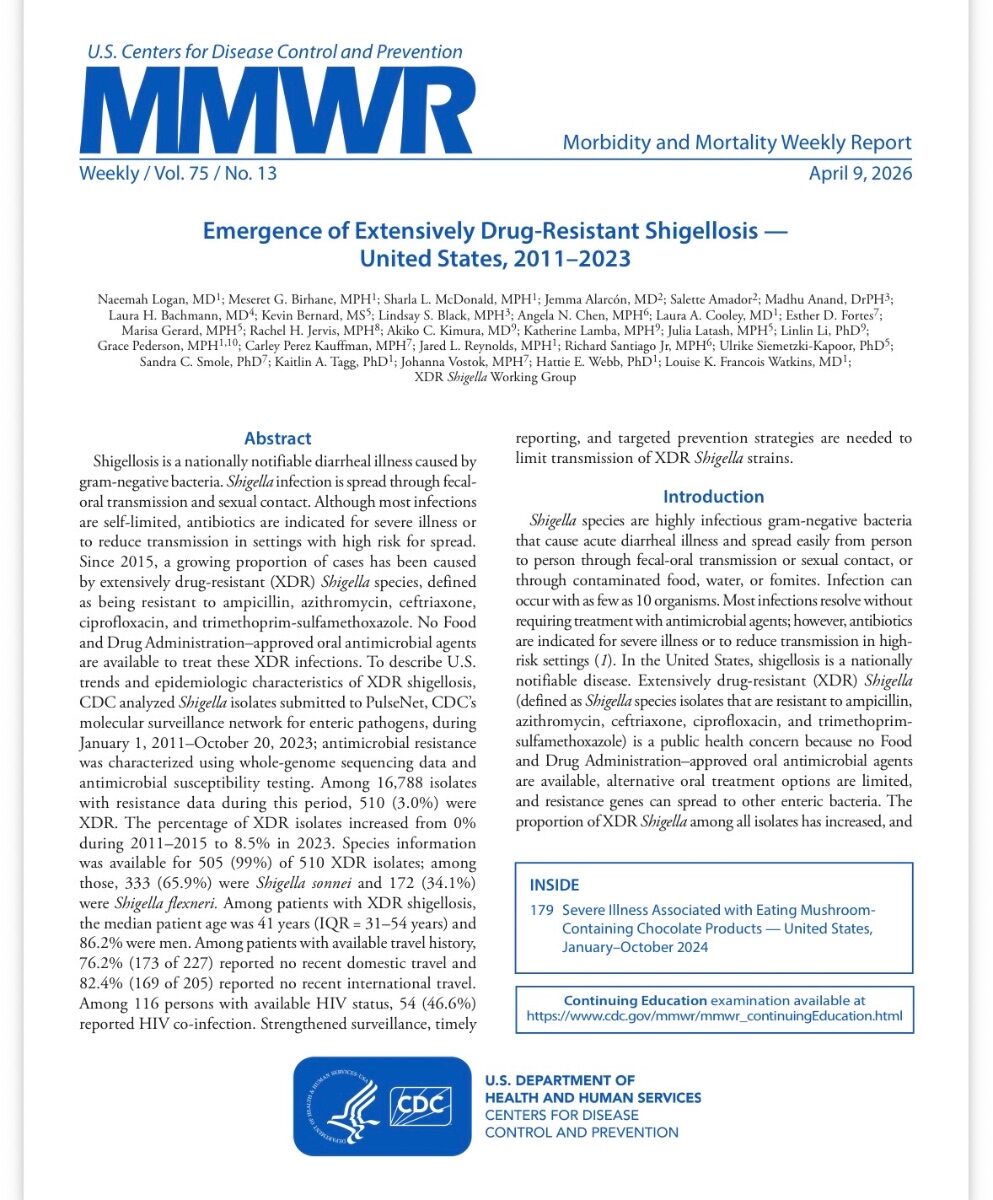
Shigellosis case incidence by general-population in my city is estimated at about 1 in 10,000-20,000 annually. Quantifying by MSM subpopulation denominator is not easily ascertained but it is disproportionately greater and there can be transmission clusters like for any susceptible group. Computed risk by specific behaviour in probability terms remains elusive. But if infection occurs, the chance that the strain is extensively drug resistant appears to be hovering around 10% based on 2023 surveillance data as reported in the MMWR piece, with proportions rising since the mid-2010s. It is reasonable to extend the upward trajectory trend since then and going forward. However, the gen pop incidence of the now two main identified strains of elevated concern together amounts to about 1 per 100,000 by simple arithmetic. Hospitalization rates in the MMWR report were roughly one in three. Since no FDA-approved oral drug treatment exists for the extensively resistant strains, the precise role of hospitalization is somewhat opaque, supportive management versus attempts at salvage regimens still under evaluation. We are seeing accelerating prevalence velocity in a disease variant that remains relatively rare in probability terms, yet still carries a meaningful chance of making one sick enough to occupy a hospital bed. Those few won’t proclaim it’s much doo-doo about nothing.
-
Without seeing the ad it’s impossible to ascertain whether the client’s logistical questions were mostly superfluous, apart from the titty-bounce specificity. Each side sought needed guiding information. Any true forensic analysis can be little more than speculative. If so many matches seem made in purgatory on Groundhog Day, then think outside of the box. Male inclination to sexual gratification that, for some, drives an erotic experience not culminating in appointments is also categorically what propels actual bookings by others. Horniness isn’t useful unless it’s imperative transcends logical control and ATM withdrawal misgivings. It’s the provider’s key resource and it’s often shallow and fickle. Don’t be a heat-seeking missile and grouse about the engineering. If vendors wish to economize on laborious setup energy output, then a detailed boilerplate response (even if seemingly duplicated from ad platform) that covers off typical inquiry content is the better playbook. A well constructed and worded mandate need not be individualized to come across as inviting. It can satisfy the type of descriptive service scaffolding that avoids legal liability. There’s this thing called ‘select and paste’, not excluding options for personalized flourishes. I once ran a consultation service. Its nature was broad enough to stimulate pre-booking questions about what to expect. That ambivalence was largely assuaged by what I believe is called in marketing terms preemptive copy, deflecting the need for hand-holding through the calendar interface. It told them what I’m cooking with and anticipated the questions that could be reasonably answered ahead of time. Very very rarely did prospective consumers seek feeling me out more thoroughly if they had taken a few minutes to read the written précis.
-
According you semantic beta-testing credit.
-
Unless the factory setting travelled here in a Time Machine from 1981, it still comes with a “some assembly required” insert.
-
Is the Secret to Men’s Longevity a Great Butt?
+ SirBillybob replied to + glutes's topic in Men's Health
One longevity-supporting thing that likely overrides booty-maxxing, seeing as glute fitness is a proxy marker for a broader cluster of health promotion behaviours, is not being in a position to extinguish butts. -
Nothing went wrong, or will imminently, unless Samantha orders the last Benedict and Anthony doesn’t particularly care for Florentine.
-
Deep-sixed onto the cutting room floor this wedding banquet scene footage featuring cast extra Debbie …
-
Normalize. Candid, playful, and confident wins the day. Bare-gummed an optional accessory package, but I would avoid hyperbole regarding the uniqueness of it, or the ‘your loss’ challenge. “I wear dentures and I give head, so I can provide the downtown experience in two formats. Nobody taking me up on my offer has complained so far.”
-
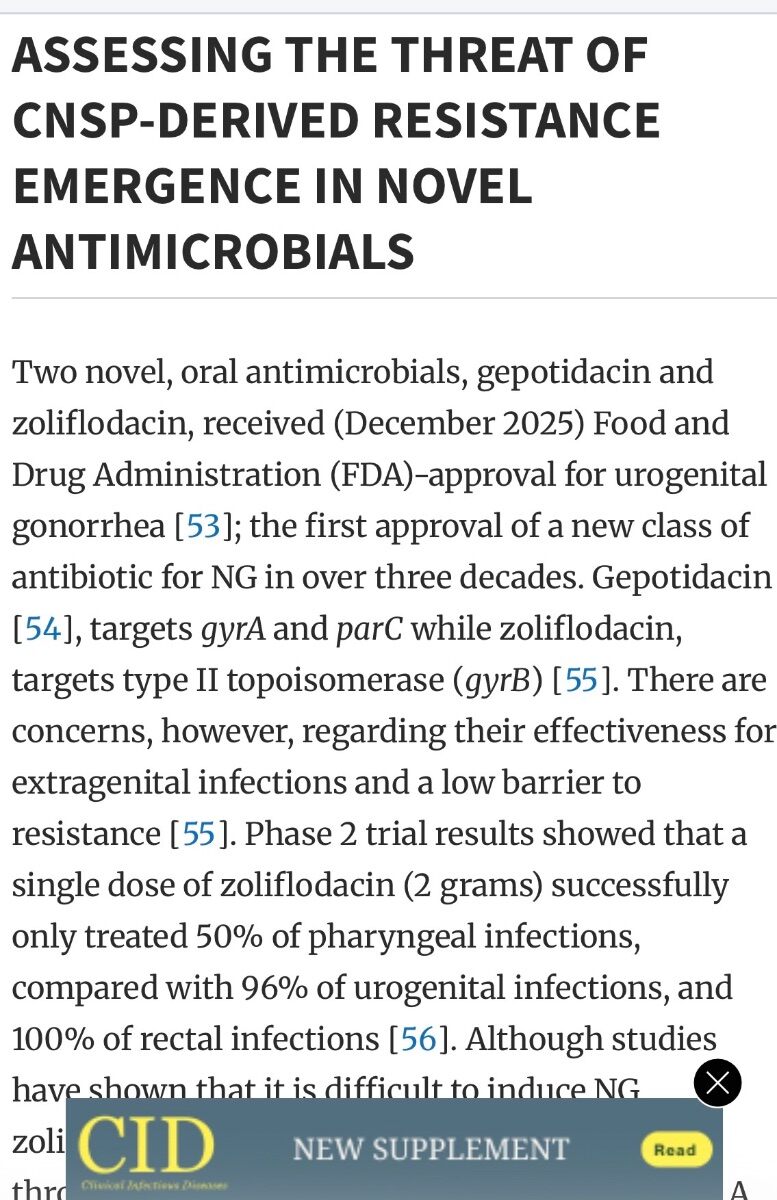
In reading the chatrooms I actually detect a fair amount of misguided reliance on DoxyPEP. Not magical thinking, that was colloquial, but a shortfall in grasping important nuances apart from irrefutable upside. Surveillance, increased testing cadence, and ongoing drug development are of course preferable to epidemiologic fog and research stagnation. My hesitation is with the subtle drift from the idea of enhanced disease visibility toward the notion of true sustainable better control. More testing can improve detection without proportionally reducing transmission. Therapeutic pipelines can exist while antimicrobial resistance realities evolve alongside them. A pair of “promising” first-in-class additions to the toolbox does not necessarily justify the degree of reassurance some seem to derive from their existence alone, particularly when DoxyPEP itself is imperfect against NG, pharyngeal infection reservoirs remain notoriously difficult terrain for the current aggregate of options, and resistance anxieties begin shadowing new agents almost as soon as they appear on the horizon. Improved diagnostic and treatment infrastructure aside, I’m less convinced the current state of affairs should be mistaken for stabilization. Pray I’m wrong.
-
Of course some news is better than no news. The two new medicines are approved for uncomplicated urogenital gonorrhea, not as a magic eraser for all anatomical sites. Even the recent reviews flag unresolved extragenital treatment failure, particularly pharyngeal efficacy, and worries about the type of resistance concerns that have plagued cure hopes. Neither zoliflodacin nor gepotidacin is being advanced for prophylaxis indication at this time. Deep throat is historically where NG therapies go to be humbled, while the least condom use understandably occurs with insertive and receptive oral. A three-decade slow crawl to the current drug milestone, not at all Infectious Diseases diffidence, might recalibrate one’s sense of how briskly the next generation of options will appear.
-
gross! A hockey show with straight couples? YUCK! ICKY-POO!
+ SirBillybob replied to samhexum's topic in TV and Streaming services
Still able use the download function and watch without commercial breaks. But 8 episodes all close to an hour? Forecast: draggy with a chance of scattered outbreaks of 10-second forward clicks. -
I once had a subscription to Stock’s webcam feature, sometime prior to the proprietor shift a few years ago. At that time a list of the night’s performers was depicted, superimposed in writing like a movie credit, at the beginning of each new shift iteration. If you set aside those few minutes from a location distance such as home you could anticipate who would eventually perform their few shift cycles. At that time it might have influenced spontaneously hailing a cab to Piazzetta a few steps away. The videographer was stationary but would sometimes zoom in on dancers chatting with customers during brief periods not focused on the stage performance. I assume most customers thought their presence could only be detected by sitting directly around the stage. The vid loop of a few operating hours would last at least 24 hours until the next live broadcast. However, some here will nostalgically recall that private dances at one time were out in the open. What is unclear to me is whether you could have been filmed in a supportive role with the dancer squirming all over your lap. One’s facial contortions as a customer, or consistently motorboating in an appealing crotch, or mayhaps an amply hooded trenchcoat, would have been the only thing supporting plausible deniability.
-
A false pregnancy.
-
Booking communication is performative but calls for practicality, style of course tied into branding, whereas service delivery is a different curated skill set. The hire may come across as cryptic or taciturn in planning, yet the session itself may prove so satisfying (or not) that any presumed halo effect linking “good DM energy” to actual meet quality starts looking less objective than originally imagined. My experiential take is dearth of correlation along with consistent predictive capability. I acknowledge that brevity in texted planning and the trend of good fortune in consummation undermines the solid determination of an association between the parasocial scaffolding and the down and dirty. For added context, mine don’t in the least charge “quite a bit”, assuming that descriptor relates to the $ figures I routinely notice within this chatroom. I expect courtesy as a mutual general standard, not a quality baked into compensation. That said, a client might appreciate a romantic and flirtatious “Will you accept this rose?” in order to seal the deal. The heart being a lonely hunter, it wants what it wants.
-
gross! A hockey show with straight couples? YUCK! ICKY-POO!
+ SirBillybob replied to samhexum's topic in TV and Streaming services
That’s what each of one of the pair in this image said …
-
Those were essentially Harvey’s own book tour words regarding her muse the ISS livestream. Her use of the analogy complicates ownership of the observation somewhat.
-
Oh well. I clicked with the mouse and the space-themed book clicked with me, a jury, and bestseller lists. “The needs of the many outweigh the needs of the few.” ~Spock
-
Fairlay Community Center (fictional)
-
Twice? Then set adrift on memory bliss?