SirBillybob
-
Posts
3,825 -
Joined
-
Last visited
Content Type
Forums
Donations
News
Events
Gallery
Everything posted by SirBillybob
-

First time travel to Brazil from July 26 to Aug 12, 2022
+ SirBillybob replied to Trundelav's topic in The Americas
Devil’s Breath? Good Night Cinderella? Place your bets. -
Infection exposure risk assessment depends on rolling local incidence/prevalence metrics stratified by the unique risk subgroup, ascertainment bias adjustment for case undercount, contagion duration, and number of (theoretical or real) contacts in an individual’s behavioural risk radius. As well as the inferred protection from artificial immunity, and perhaps considering an estimate of recent natural immunity breadth per risk-group capita. With all these variables one can approximate a numerical probability of exposure, if not infection fruition, and stack that up against one’s risk tolerance. If only equivocating about vaxx uptake at a binary level and not considering these factors I don’t see the point in much discussion. I am not going to data dive into all of the variables but I do follow incidence as @Unicorndoes. I will have a fair sense of reasonably quantified exposure risk for my winter SoAmer extended sexcursions, as I will plunge into the available data in several weeks when relevant. I am paed Vaccinia scarified and had a primary MVA-BN dose subQ in June. I’ve had 2 automated reminders for 2nd dose subQ but passing for now. Knitting the factors together, risk is statistically low. The important thing is, while incidence is now reduced and vaxx uptake high in NoAmer excluding MX, where you travel may have incidence not reflected in regional epidemiology data. Also bear in mind that in some regions there is minimal artificial immunity (eg, no MVA-BN uptake) and the ratio of natural and artificial immunity is unknown. If somebody wishes to convey sound estimates of the variable gaps above I have not investigated, I can provide some examples commensurate with the algorithmic applications that underpin exposure risk by N people, and that were utilized by, but basically ignored, Georgia Tech U and Stanford U’s efforts for SARS-CoV-2. Technically, it’s more simplified because risk is group-specific, visible manifestations spur assortative behaviour, and MPXV is comparatively wimpy viz transmission. This is unrelated to vaxx SAE considerations.
-
First time travel to Brazil from July 26 to Aug 12, 2022
+ SirBillybob replied to Trundelav's topic in The Americas
Unfortunate, and all too possible though likely statistically rare for once in a lifetime visitors whereas your risk is inflated temporally. So far, having accumulated several months in Rio/Sampa since 2015, I am incident-spared. My playbook is, similarly, to not appear the least bit infected with affluenza. May I ask the general location of your mishap? -
I myself would more than welcome a crack at dawn and in my mind’s eye it would be imbued with a heavenly very arousagenic light. He might be the actual sole trash in the bedroom while it is unlikely I would be deemed such. 😌
-
He (Theo James) sucked himself off via time travel in a previous series; now somebody else will likely need to step up.
-
It’s often as simple as mechanical friction. So, reparative sexual conversion camp?
-
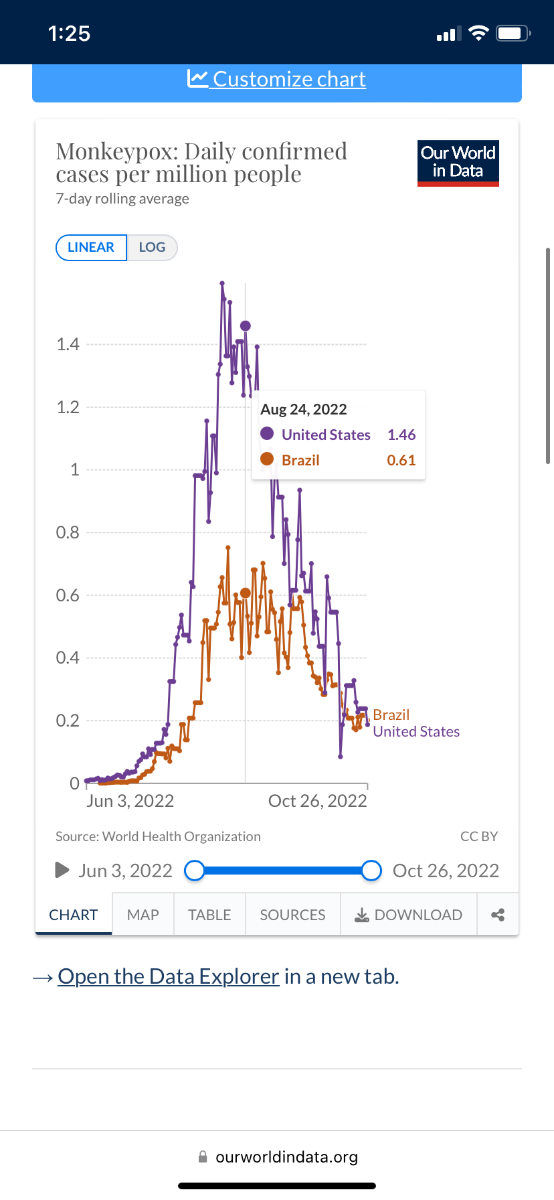
Curiously and crudely, Brazilian MSM make for an interesting non-MVA-BN-uptake observational comparator group. I sliced in at Aug. 24th as that is when Brazil launched a more elaborate public awareness campaign. The main incidence epicentres had been very up to speed very early on in terms of health professionals’ awareness of disease presentation and diagnosis. Begs the question: was immediate rolling natural immunity among high infection susceptibles and dispersers going to cut it on its own, eventually burning out spread just about anywhere?

-
Monkeypox is so last season in Quebec. Currently elevated incidence of paediatric RSV is pushing children’s hospitals to the capacity brink, what with disease season moving in.
-
Another article making the rounds this year in epi circles, notwithstanding the reality that it was apparently very deeply peer critically appraised prior to publication, ensuring that all limitations were accounted for, would seem to provide to the average person with basic science literacy a convincing argument that the null hypothesis of wearing effect is not definitively not rejectable. There is likely a population subgroup that is fully aware of the changing picture and has decided that wearing not be abandoned or that wearing be context-specific … for them. Therefore, a HCW conference, airline flight, etc pattern of uptake is transcended and, as mentioned, the wearing standard in certain settings bleeds into other settings. They may even be aware of the futility of attempting infection prevention and source transmission control without majority uptake reciprocity, while cognizant that the evidence for benefit remains unfounded. This might be described as maintaining comfort in a position despite ambiguity. https://www.pnas.org/doi/10.1073/pnas.2119266119
-
Well the efficacy (9.5%) compared assumed that baseline wearing controls remained 10% pop’n usage and that intervention wearing was about 40%, with a consistent differential of 4-fold. However it would be akin to taking a state the size of Bangladesh (eg, Georgia) and cluster-randomizing in 600 (300:300) geographic pockets where mask allocation pockets and control pockets are in close proximity yet with, it’s hoped, no cross-contamination of wearing rates. Analogy-wise, a more robust design would compare, say, Georgia and Michigan, and would increase the differential in mask-wearing uptake. [Thoughts about cooperation should one or the other be allocated masks for all with an offer to contribute to science?] So it’s not a nice and tight RCT design and it’s difficult to reconcile the relevant infection acquisition variables in terms of whether the approach subverted a truer or better wearing effect or lead to a spurious result. This would be an example, perhaps, as @Unicorn has mentioned regarding research overall, where the result suggests feasibility of further investigation. The problem, however, at the risk of beating a dead horse, is designing a RCT with an incontrovertible binary (usually dichotomous) intervention. Health care workers, for example, if they are the research pool for comparing PPE variations, acquire infection attributable to settings (eg, household) where PPE is not utilized. If vaccinated, in contrast to unvaccinated, they have the clinical effect stabilized on any given day irrespective of life setting. Similarly, for Bangladesh and elsewhere, masking is not always consistent or used where risk is highest. The self-selective differential within the current genpop minority of voluntary wearers, between N95 and procedure (have I got that right? latter = surgical?) versions, as well as wearing or not and context-decided, and so on, is not surprising because the total body of research, including PPE behavioural and ecologically mechanical, etc, has not heretofore been summarized and integrated into a cogent consumable format for the public. Even here, the information is scattered and fragmented through nobody’s fault, often personalized, peppered with N=1 anecdotes, and contributed in repeat topics. It is like a microcosm of the challenge for the overall community to interpret and decide what guidance applies. It’s like trying to track the written minutes of related topic seminars jumping from academy to academy and school term to school term. As far as the question of face covering type, there seems often to be a piece of research that cracks open the ongoing discourse and calls for renewed attention, suggesting a hierarchy of relative PPE protection, or when in the pandemic trajectory a tactic might be more or sufficiently worthwhile, and so on. And always non-controversial and cool-headed, right? One making the Twitterverse epi rounds more lately suggests that the possible hierarchy explored is comprised of mask format, facefit-integrity, and the supplement of mechanical air filtration extraneous to wearing. One sentence describes the lack of difference between fit-fail N95 and surgical (fitfail by default, I think), highlighting that N95-fitpass is prophylactically superior within the hierarchy. To my way of thinking, some folks may erroneously interpret that as N95 superiority because subjectively the tendency is to perceive that its fit is snugger. They are not about to cart around portable generators and the information is packaged in such a way that a hierarchical gradient of positive effect exists, hence, some possible benefit is inferred as a heuristic: mask wearing is helpful, yet the essential difference (ie, none evident) in mask type is sublimated. The N95, then, is extrapolated as better. This is just one example of people attempting to mitigate risks to health and continuity of daily life (ie, avoiding infection-poz adjustments) through trying to make sense of what might work. https://academic.oup.com/jid/article/226/2/199/6582941?login=false
-
It’s important to distinguish between public health recommendations for mask mandating and masking itself. Some entities have decided that the trajectory of COVID morbidity, lethality, extended post-recovery chronicity aspects what have you, are not particularly helpful in underpinning a dichotomous message, because people need a simple directive and the public will often consider such variables in individual decisions anyway. Quebec’s singular message is that masks reduce the risk of SARS-CoV-2 infection. Period. Crickets on face covering format; so be it. Notwithstanding that the null effect hypothesis is neither convincingly upheld nor rejected, there exists a small body of observational research that maintains tension between the possibility of some benefit versus no benefit. The contextual mandate of masks in certain settings in the province reinforces the view of some benefit albeit unsubstantiated at a rigorous research level. The impediments to executing robust research designs aimed at resolving the question at a basic binary level, according to some public health entities it seems, are not deemed to justify a dismissal of a null hypothesis result directionality that favors masking as a legitimate mitigation measure. The paradox itself, the lack of supporting or refuting data because such data are elusive, doesn’t establish a basis for a recommendation one way or another at the individual level of self-determination, of choice. In Quebec, probably elsewhere, rounding up to the assumption of salutary effect in certain settings is going to spill into individual preferences in people’s overall ecology, such that they will extend a central message of mask utility and round up behaviourally elsewhere, though not obligatory, yet possibly extended to the idea of protection and infection source control for a grouping of pathogens. The higher rate of masking among older folks may be, in part, an artefact of the actual mandate in health settings with which they are more likely to intersect. I don’t see how the decision to mask is contradictory for any one single Québécois, whether trustingly following the public health bottom line or having drilled down, data-dived, into the pool of extant research.
-
This should go well. 😉
-
This starts out sounding like the ophthalmologic equivalent of walking down dark stairs in a horror movie; glad the ending was happy.
-
I thought Tony Orlando & Dawn had it down. If your dick is whacked twice it’s a hard no. If the top of your palate is banged a few times according to the predominant agenda the other party’s interest will have been evident.
-
For old geezer Canucks like me, this depicts regions you are likely to access the higher dose of Fluzone automatically depending on your category within a jurisdiction. In some regions you would need to request it and pay a fee, maybe $80?, if it is even dispensed where you attend. If you are taking Fluzone as your vaxx at no cost (there are other products approved as well) and wish to double-check the formulation the pre-filled syringe is 60micrograms/0.7ml… standard dose is 15micrograms/0.5ml. I take the standard dose. The CDC adjudicates the evidence as favourable but of low certainty grade, consistent with the research I have been reading. Not sweating it; pun intended. Happy poking.
-
Those providers. Give them a few inches of your rectum and before you know it they’ve taken over your home.
-
Actually flu vaccine was, surprisingly, available in Quebec as early as Oct 5th. Ontario officially Nov 1st but obviously has started in places. There may be other provincial inconsistencies and the national immunization guidance would give most people a headache trying to wade through it. I received a standard dose Fluzone Quadrivalent in spite of being of age for a higher dose (4-fold greater concentration and possibly modestly more efficacy). I’m not concerned. Apparently Quebec is reserving the higher dose for long term care settings. But I think the CDC recommends the higher dose for 65+. Canada indicates it can ONLY be given to seniors but isn’t being fussy about it being a strong recommendation. I believe it’s based on Sanofi’s research of a few years ago that showed a higher dose trivalent outperformed a standard dose. I think the difference in breakthrough illness risk was 1.4% versus 1.9%. I’ve never taken a ‘sommelier’ position on flu vaxx and not going to start now, though “THE flu shot” is a misnomer. But what products provinces select likely impacts on delivery to some extent, along with the many moving parts of attempts to pragmatically conjoin two Fall vaccination campaigns. Funnily, imagine the Twitterverse imploding if these ambiguities were specific to COVID vaccination.
-
I had posted elsewhere I usually didn’t access flu vaccine in Canada as early as October and usually paid a fee in spite of senior status, but low and behold it rolled out early in Quebec this year, and free for age 60+, so I received it yesterday. Simultaneous admin of COVID vaccine is likely saving on manpower, but pharmacies here can only cold-store Spikevax and the Moderna BA4/5 is just submitted for review. Besides, I have consistently been sent crawling into bed with fatigue malaise fever etc following all COVID shots and wanted to keep separate for attributing possible reactogenicity (though merely once out of about 40 lifetime flu shots did flu vacc send me crawling into bed with shivers). I was feeling fine 24 hours after flu shot and at that point walked in to a vaccine centre (today) for the preferred Pfizer/BNT Comirnaty BA4/5 bivalent booster, offered a choice against Spikevax bivalent BA1 … Already feeling woozy a few hours later. And the pharmacy where I got flu vaccine flagged that I am eligible for free pneumococcal vaccine, on top of the email notice of eligibility for 2nd Imvamune dose I just received. Aren’t these threads all sounding like they’re from some post-apocalyptic script? Will that be your right or left pincushion that we plague today, monsieur?
-
AFAIK no gold standard placebo-control randomized clinical trial officially registered, just a large-ish observational cohort in Spain where subjects have self-selected for MVA-BN. Prospective incidence over 6 months but with it currently really tamped down. And the small dose-sparing noninferiority comparator trial in USA, only 70 subjects in each of 3 arms, and immunogenicity only … there we go again, only inferences possible.
-
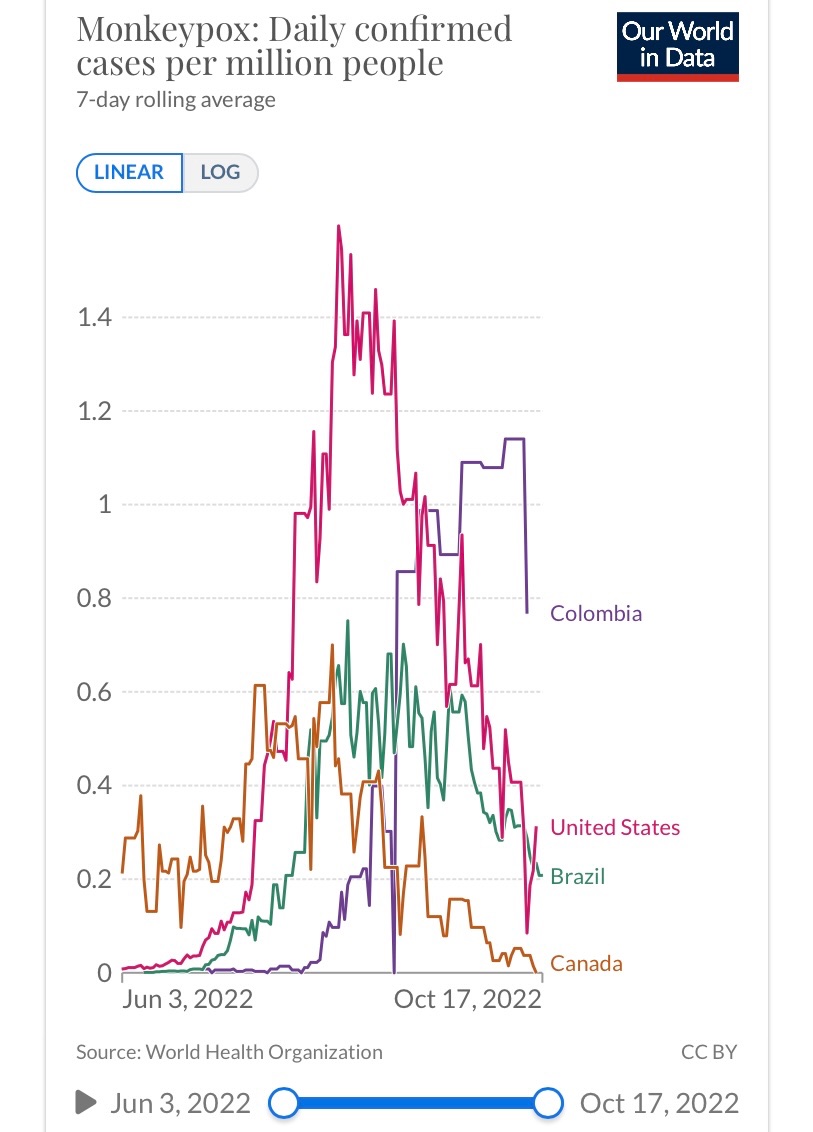
I also received the Quebec 2nd dose prompt. I am sticking to my plan to hold off as an older childhood smallpox vaxx recipient. My main concern would be wintering in Colombia/Brazil as usual, but case incidence appears to be self-limiting even without vaccination access. Running its course, altered sexual behaviours, vaccination impact irrespective of the first two factors, who knows? I may need to adjust expectations for infection avoidance given a focus on sexual interaction when there.
-
This article nicely summarizes the breaking research … some of which has already been touched on wrt this thread… https://www.aidsmap.com/news/oct-2022/monkeypox-vaccine-appears-effective-studies-have-mixed-results
-
Covid vaccine increases death rates!
+ SirBillybob replied to Alex.Blessings's topic in Men's Health
It’s a clinical heuristic that was not unreasonable, particularly in the face of contrarian resistance and wackadoodle assertions by politicians. Additionally, a transmission component could not be integrated in early vaxx research and the expedient was efficacy. Pharma did not indicate transmission impact was zero. It called for more complex research design. The first step in reducing viral transmission is to reduce infection. If we lacked the sophistication to assess transmission potential in spite of vaccination, the incidence outcome would have nevertheless supported the inference of both prophylaxis and reducing spread. Moreover, the research supports that transmission was attenuated. But if you want to obsess and discount that vaccination’s overall success story is bunk, unimpactful, that the mandate’s benefits did not override downsides … What is more inaccurately revisionist? That early intervention messaging was framed in a manner that yielded no beneficial effect on overall pandemic morbidity/mortality due to well-intentioned wording emanating from slack uptake, wording that is now fallaciously viewed as outright mendacity, or that breakthrough infection, already known from the get-go, retrospectively invalidates the benefits assumed and desired in the first place? Both are flawed, and false dichotomy. The virus has adapted to many changes without its own scapegoating finger-pointing council of naysayers; we need to roll with changes in info as well. -
Covid vaccine increases death rates!
+ SirBillybob replied to Alex.Blessings's topic in Men's Health
Fake-ish news. Why current testimony is required is inane. The original FDA submission, in the public domain and which I read 22 months ago, made no claim regarding transmission. People wanted a rose garden so much that they believed it was promised. It wasn’t. We are essentially in a situation consistent with the early attempts at supportable evidence released 22 months ago. Some folks will go to the mat to justify a perception of being put-upon-pie Georgie-Peorgied. Show me where this victimization theme is evident in LMICs. Even if transmission claims were alluded to by entities extraneous to Pfizer/BNT they were subsumed within guidance that the salutary benefits of vaccination were solid in terms of attenuating poor CoV outcomes. An obsessional false dichotomy between disease reduction and transmission simply and sadly undergirds this victimization, undermining uptake and its irrefutable benefits.
-
Covid vaccine increases death rates!
+ SirBillybob replied to Alex.Blessings's topic in Men's Health
Fauci is irrelevant to the majority of the world, including me. I don’t pay much attention to USA news or visit. I doubt the blood bath south of our border is attributable to him, or that the most pristine and semantically correct or optimally worded projections would have contributed much to the variance in outcomes. He is a convenient scapegoat when whoever was in that position was a proverbial Sisyphus. Would I hang him out to dry for not accurately second-guessing the host’s MO? I don’t think so. Stop? Slow? Who doesn’t want an unequivocal answer. The problem is expectations and entitlement. How could you design a transmission research study then now ever? Too many confounding variables contributing to the variance in the binary logistic regression inferential statistics. Infection exists or doesn’t at any point in time in an individual because it simply got them. The reasons are multi factorial. You cannot isolate the myriad of contributions to exposure and infection in the way that vaxx vs placebo is dichotomized in RCT. For example: scores of two person households; 1:1 assignment, half of pairs where 1 provided artificial immunity (primary, boost, what have you?); half of pairings neither immune at baseline. Pairs are not isolated silos. One non-immune or immune could have 100-fold outside contacts compared to another. You cannot control for, hold constant, all the factors that swirl around the central question: does a vaccinated individual transmit virus yielding infection to another? All that can be determined is that infection is possible, and we already know it. That better outcomes are underpinned by transient quantitative immunity. If it were, say, a prospective design of 10,000 theoretical households over 3 months, capturing the typical 1% rate of cases (100 in this case) how many antigen tests? Daily? 1,800,000 tests in the budget? What chi-squared analysis even if not multivariate? What variables loaded into a multivariate logistic regression model? And where are you going to get completely non-immune households at this juncture? Do you think vaxx negativists will line up at the recruitment depot? These conundrums don’t make Fauci a limited dumb fcuk. We’re all limited lame ducks. The pandemic blind is too big. -
Covid vaccine increases death rates!
+ SirBillybob replied to Alex.Blessings's topic in Men's Health
Another logical fallacy: false dichotomy. It’s only absolutely untrue that spread is reduced if there is no vaxx benefit conferred in terms of mitigating morbidity AND duration of infection. It is incontrovertible that morbidity is reduced by vaccination. “Stopping the spread” is a logical and common colloquial generic usage to underscore desired improvements in outcome. This constant conflating of public messaging regarding the salutary benefits of vaccination with devious misrepresentation intent, as vaxx yield was not accompanied by hoped for transmission elimination, is illogical. Infection is not dichotomous viz transmissibility, as if the same reproduction or attack rate results within a vaxx-saturated context and a vaxx-impoverished one. Immunity is on a temporal gradient. Host infectivity is on a temporal gradient. As illness duration is truncated, transmission window narrows. Less contagion, less exposure, less incidence. Putting forward that the only reason to support vaccination were to be sterile immunity falsely dichotomizes the intervention as if it could only be entirely valid or illegitimate.