SirBillybob
-
Posts
3,822 -
Joined
-
Last visited
Content Type
Forums
Donations
News
Events
Gallery
Everything posted by SirBillybob
-
After all …

-
No. Yes. Binge first. Ask questions later. Final word on the subject.
-
That tracks.
-
June 2024. Period. For Men’s Health Month June. A stand-alone release. The current regular issue is Austin Butler. ScreenRecording_10-22-2025 20-41-15_1.mov
-
It’s Issue 7, 2024 (June 2nd). I think it’s just a special supplementary issue put out as a one time thing but not annually and, unlike the regular bi-monthly issues, does not feature a “celebrity” for cover photo.
-
Bleau Dry Station in The Village … ScreenRecording_10-22-2025 09-17-59_1.mov
-

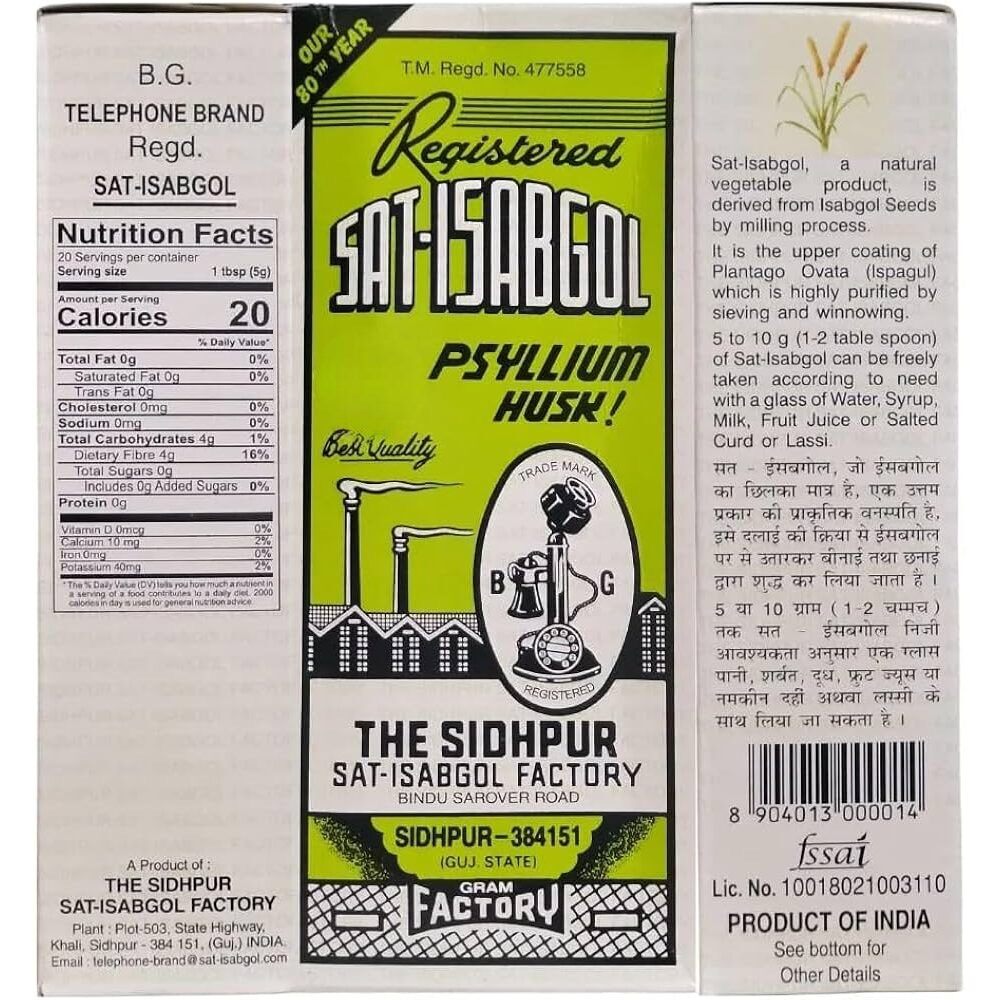
Opinions from Foodies wanted: Unflavored Psyllium Husk Idea
+ SirBillybob replied to + Just Chuck's topic in What's Cooking
From India, basically same as what I use but mine is also packaged there. I do find that if you drink it very quickly after mixing it goes down easier and the solubility process, that otherwise amounts to sludge if you leave it too long in the glass to absorb all the fluid, finishes in your gut. Straight up in water? Fear is not a factor for you.😛 -
I seem to have lost only a few of 525,600 membership minutes.
-
The site isn’t working for me going to it directly, whether rent dot men or rentmen dot eu. I have Premium. It recognizes my profile name I guess because I permanently log in, but nothing else is functioning. It labels my plan as Basic but I am able to pull up payment history delineating Premium status! —— Resolved shortly afterwards.
-
Opinions from Foodies wanted: Unflavored Psyllium Husk Idea
+ SirBillybob replied to + Just Chuck's topic in What's Cooking
As we say in Quebec, De gustibus non est disputatum. Of course, stir, whisk, blend, sprinkle to your taste … in the most delightful way.
- 16 replies
-
- 1
-

-
- fiber
- cleaning out
- (and 2 more)
-
Opinions from Foodies wanted: Unflavored Psyllium Husk Idea
+ SirBillybob replied to + Just Chuck's topic in What's Cooking
As well as where your gastroenterologist advises sufficient psyllium dosing is obtained with or without stealth and true grit. Mine swears by this imported product and uptake method I obtain in a South Asian run convenience store steps away because I have not been able to find the equivalent other than in a Rio de Janeiro bulk goods by weight shop when visiting.
-
Opinions from Foodies wanted: Unflavored Psyllium Husk Idea
+ SirBillybob replied to + Just Chuck's topic in What's Cooking
There are two consumables that won’t ever be successfully camouflaged in a Michelin star dish or a signature cocktail: cod liver oil and natural psyllium husk. My failsafe method for years for downing the sludge that results from mixing psyllium in water is to flavour the water with a small amount of low cal Crystal Light powder from KraftHeinz. A little goes a long way to make swallowing it more bearable. I hope the additives aren’t IBS triggers, though.- 16 replies
-
- 1
-

-
- fiber
- cleaning out
- (and 2 more)
-
Being haled into such fast moving plot lines it’s hard to predict events in advance.
-
I know a few young Montrealers that attended the massive annual Louder Than Life Festival last month and the city has to feed an additional quarter million metalheads on top of its local population. They did not dine out between moshings, though, as such. You might look up the range of mobile venue vendors associated with established eateries although those vendor popups are long gone. Of course you can always check out Tripadvisor’s Top 10. Kat’s Cat Café is no more.
-
For those considering the new hotel tru by Hilton be aware that another building essentially sharing a full wall is also going up, so expect major construction noise with the foundation dig &c. The plan was always an integrated project with the hotel going up first. The second part underway is commercial and residential.
-
Eaton’s Bldg … Are you aware that a bar/restaurant was re-opened on the 9th floor last year? It looks posh and I felt too casually dressed to go in for lunch when running errands and swinging by to gawk this week, although many were in jeans etc, and the hostess offered to seat me. Soon. Le 9e, aka Restaurant L’Île de France. Perhaps you had a dressy family outing up there in days gone by, well before it had previously closed in 1999.
-
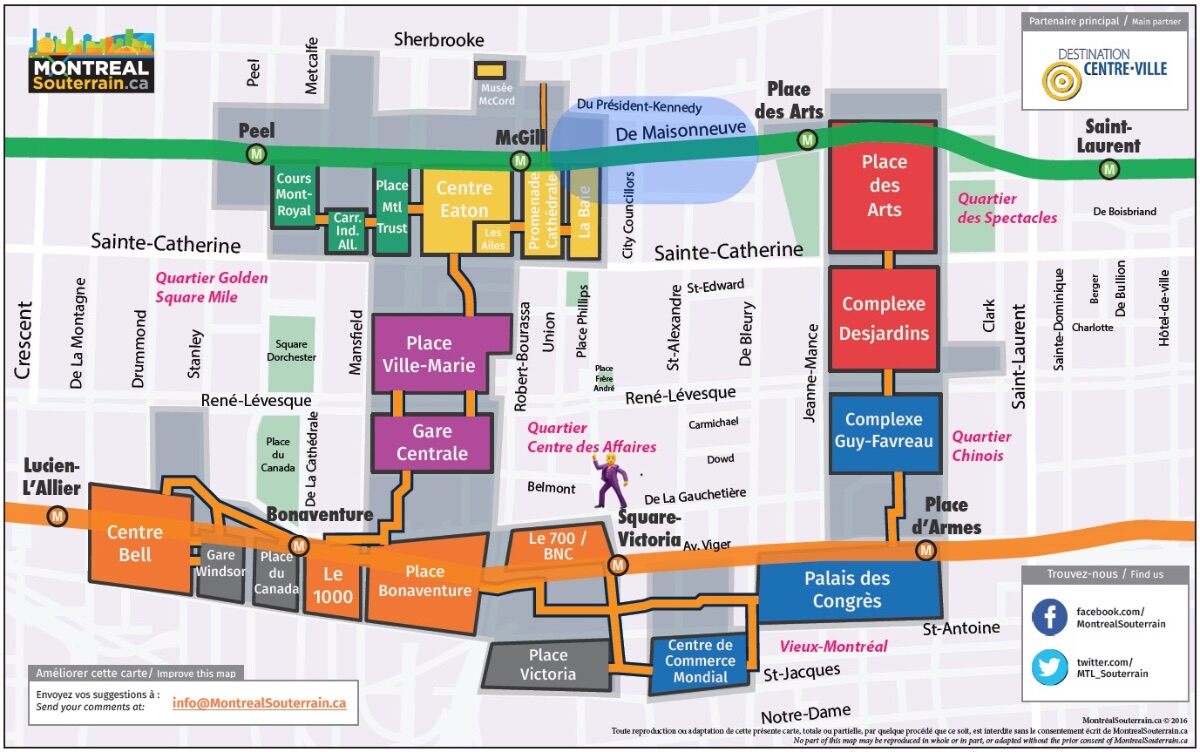
… but your phone map apps will do you little good. This map might. Little do visitors know, say, arriving at Central Station on ViaRail or Amtrak, or one of the Metro subway stations conjoined to the underground passages, that they can sometimes cut down on outdoor trekking and wear&tear on luggage wheels while getting to their destination or bridging distance between walking transfers. I put a blue shaded oval representing one of the very view breaks in the network necessitating facing the elements. Sadly, the gay strip club, lower centre zone, closed some time ago. We need to lobby prospective bidders for the gargantuan recently shuttered Hudson Bay Company flagship store (La Baie) to slip one in when redeveloping the structure’s interior, etc (Henry Morgan Bldg, 1891).
-
At Union Avenue. Henry Birks & Sons Building (1894) and Christ Church Cathedral (1859)
-
Hot New (Gay) Hockey Series on CRAVE: Heated Rivalry
+ SirBillybob replied to dutchal's topic in TV and Streaming services
-
Not fitness cooooooach?
-
Hot New (Gay) Hockey Series on CRAVE: Heated Rivalry
+ SirBillybob replied to dutchal's topic in TV and Streaming services
In the book it’s Montreal Voyageurs and Boston Bears. -
Saw daily … now that’s overdoing it.
-
Oct. 26 Sounds like all the posh English accents have rubbed off onto McGovern.